
Tuberous Sclerosis
Tuberous sclerosis is a rare neurocutaneous multisystem autosomal dominant genetic disease that causes non-cancerous tumours to grow in the brain and on other vital organs such as the kidneys, heart, liver, eyes, lungs and skin.
Station Instructions: Assess this 50 year old gentleman presenting with a rash and a history of seizures.
1. Key History‑Taking Points
Neurological History
Seizures:
Type (focal seizures, drug-resistant?)
Age of onset
Development:
Any delays in walking, speech, or learning?
School performance
Behavioural concerns (autism, aggression, ADHD)
Systems Review
Skin:
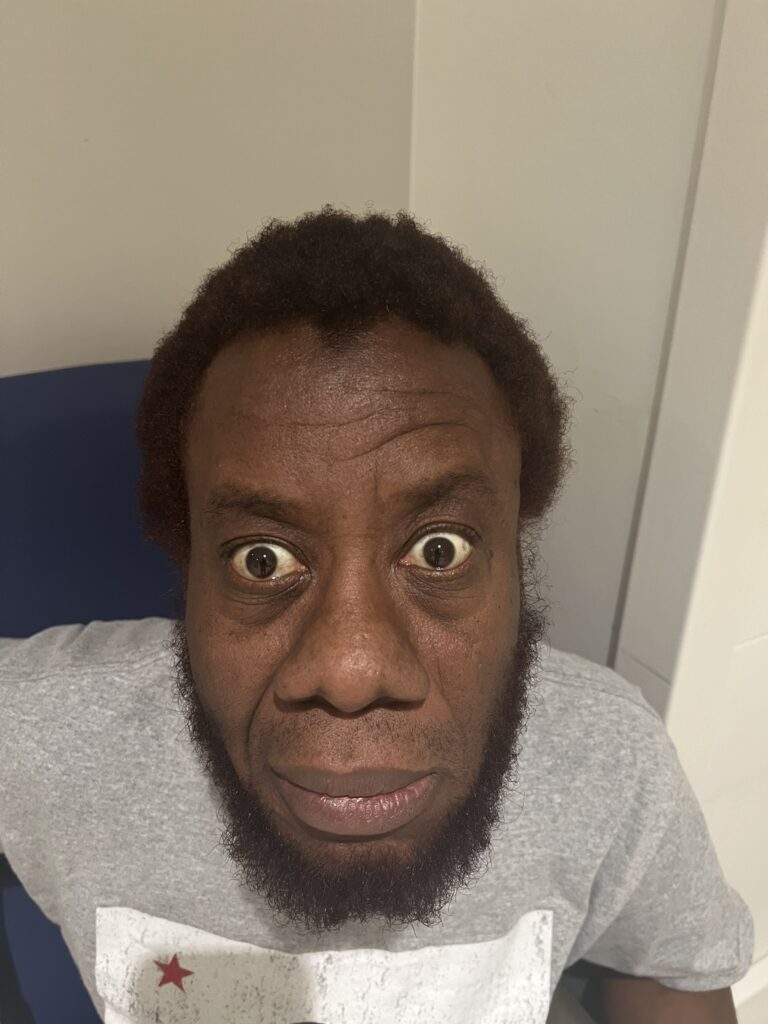
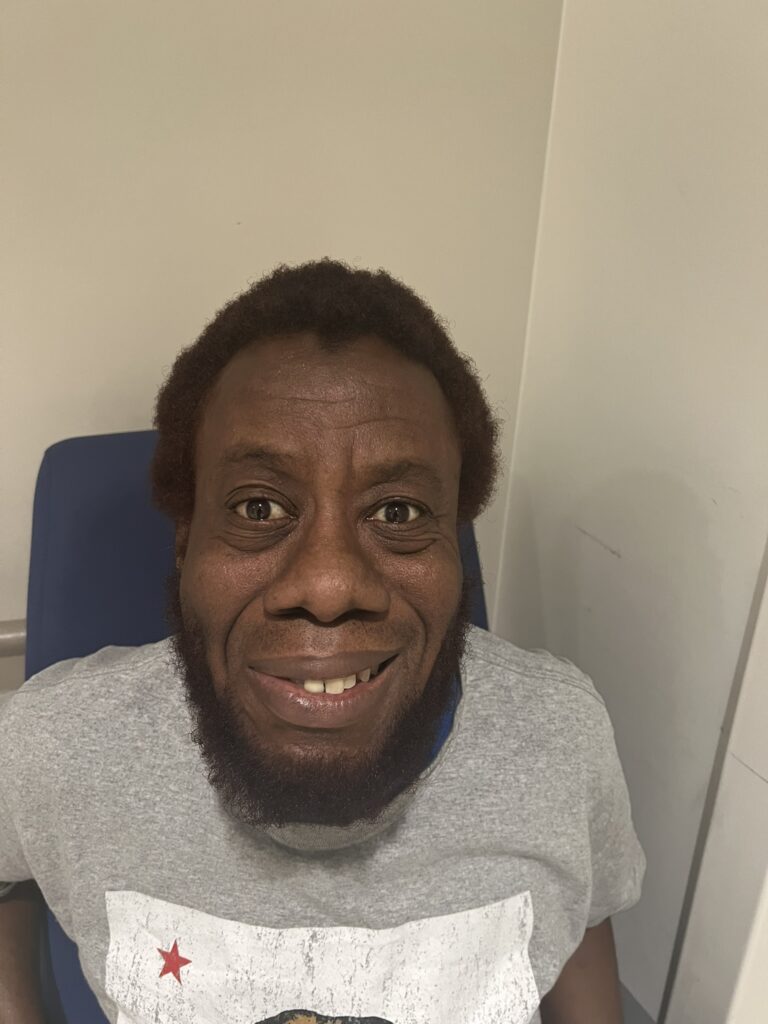
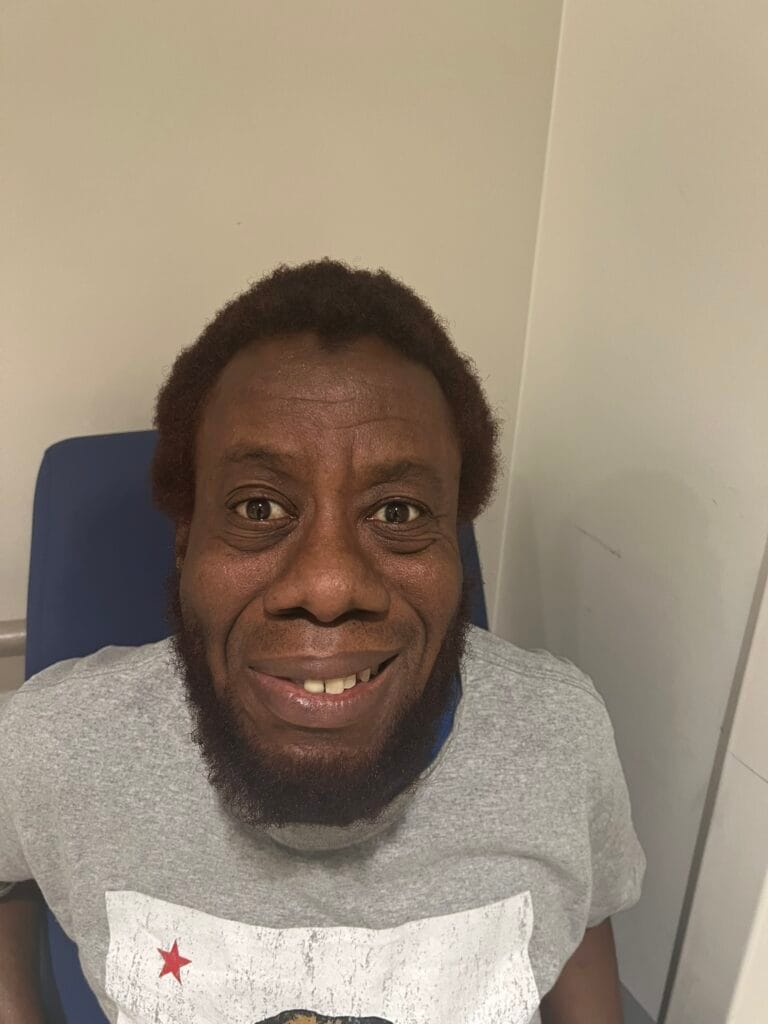
Facial spots? (angiofibromas)
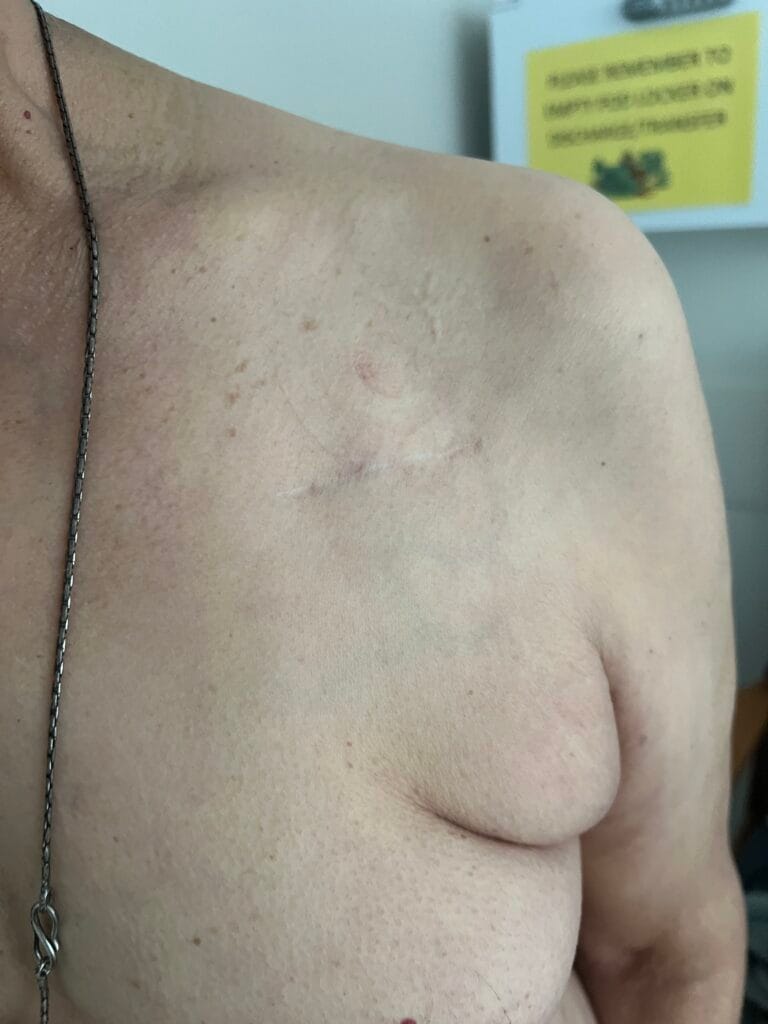
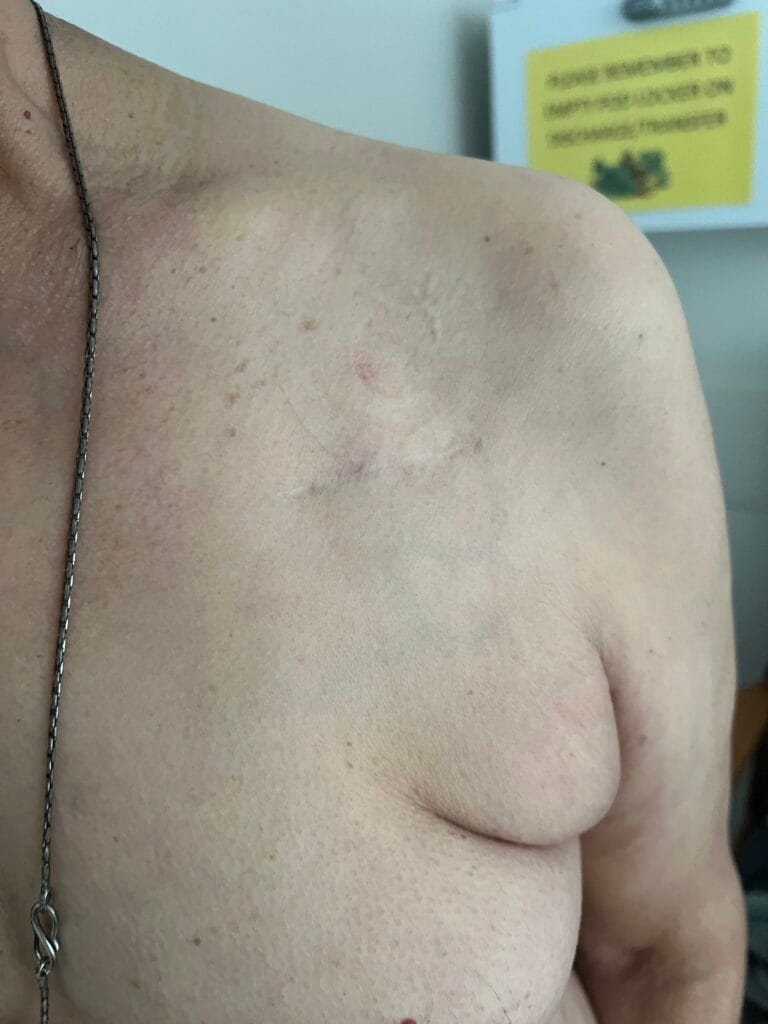
White or hypopigmented patches? (ash-leaf spots)
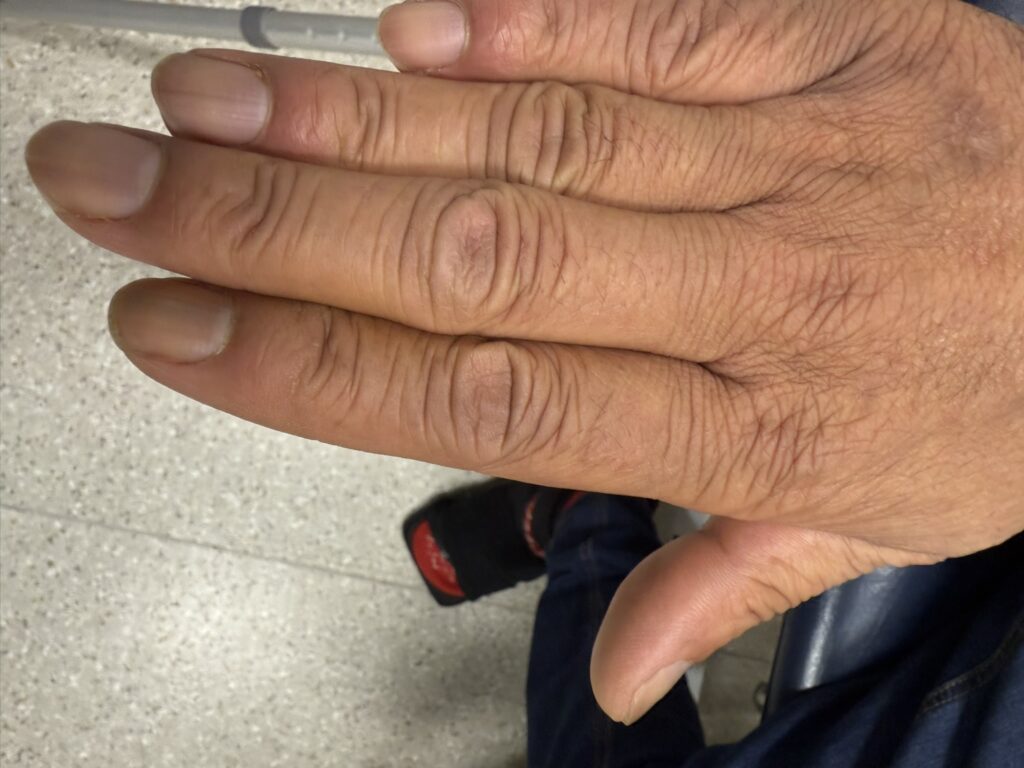
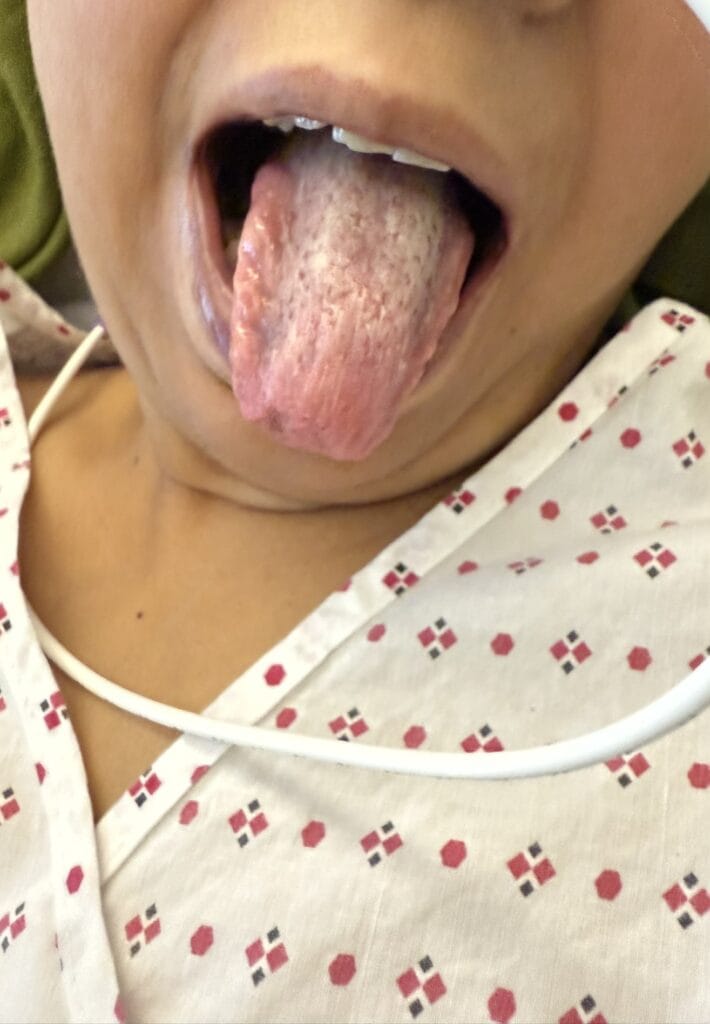
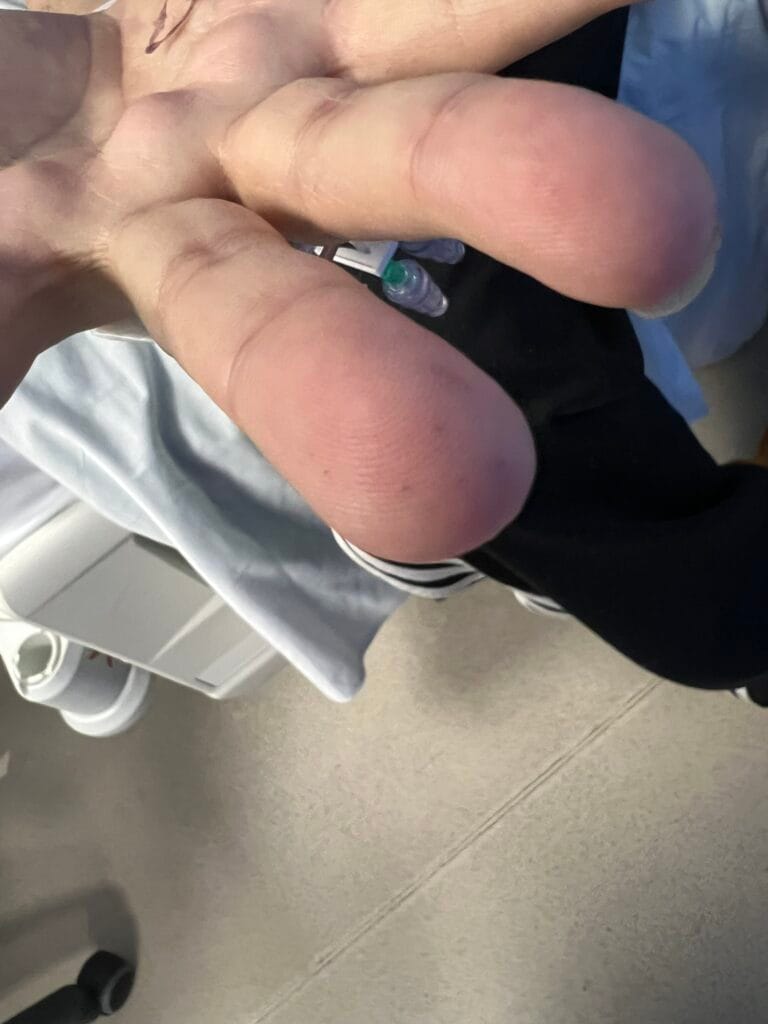
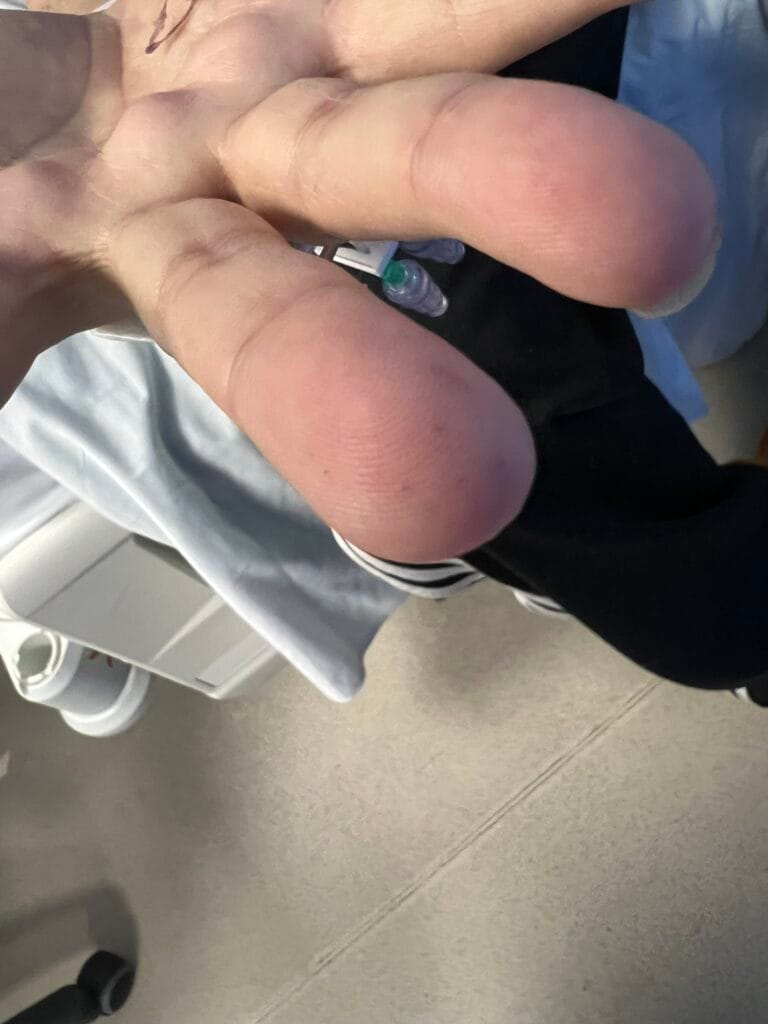
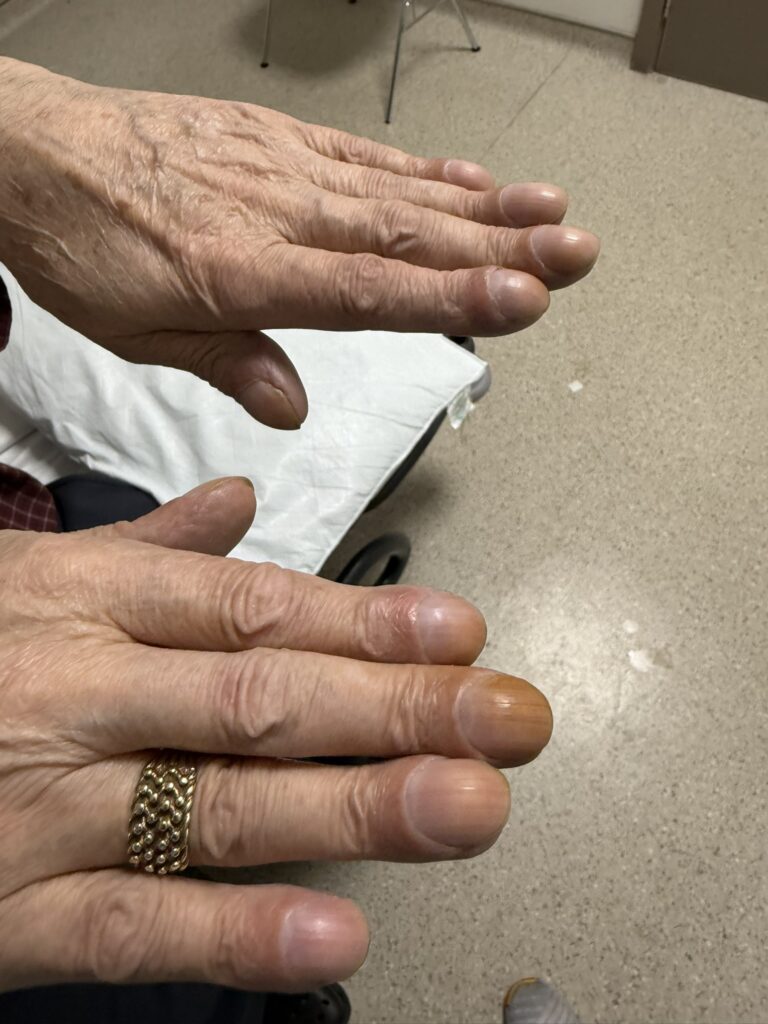
Nail or oral lumps? (periungual fibroma, intraoral fibromata)
Kidneys:
Blood in urine?
Flank pain?
Ankle swelling? (renal failure)
Respiratory:
Breathlessness, previous hospital admissions with SOB? (recurrent pneumothorax)
Cardiology:
Palpitations, fainting? (arrhythmia rhabdomyoma)
Known murmur in childhood?
Family History
Any relatives with:
Seizures or epilepsy
Learning disabilities or autism
Facial skin lesions or known diagnosis of tuberous sclerosis
Any genetic testing or counselling done?
2. Key Examination Findings
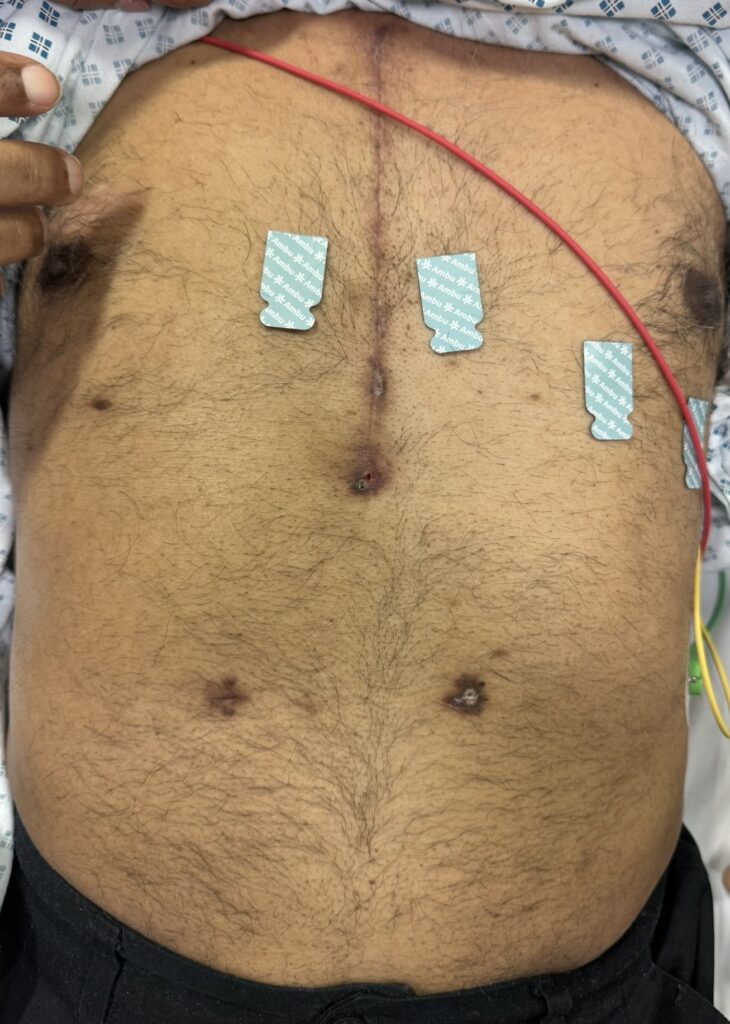
Skin:
Hypomelanotic macules (“ash-leaf spots”) fluoresce on Wood’s lamp (~ 90%)
Facial angiofibromas (butterfly nose/cheeks), shagreen patch, ungual fibromas.
Cardiac: murmur or arrhythmia suggestive of rhabdomyomas
Abdominal: palpable or BP‑related signs of renal angiomyolipoma, AV fistula or scars from dialysis
Respiratory: signs of lymphangioleiomyomatosis (shortness of breath, pneumothorax)
Neurological Examination: Focal neurological deficit
3. Specific Investigations
Initial if suspect TSC:
Brain MRI: look for brain haemartomas, cortical dysplasia, subependymal nodules (SEN), Subependymal Giant Cell Astrocytoma (SEGA)
Echocardiogram + ECG: for cardiac rhabdomyoma/arrhythmia
Skin exam under Wood’s lamp: ash-leaf spots fluoresce
Abdominal and Renal Ultrasound with renal function tests: for angiomyolipomas, polycystic kidney disease
Pulmonary: high-resolution CT and pulmonary function tests for lymphangioleiomyomatosis
Ophthalmology: dilated fundoscopy for retinal hamartomas or achromic patches
Genetic testing if not performed (TSC1/TSC2 mutation testing)
Surveillance ongoing:
Brain MRI every 1–3 years until 25 years if no Subependymal Giant Cell Astrocytoma (SEGA)
Annual Tuberous Sclerosis Assosciated Neuropsychiatric Disorders (TAND) screening and EEG as clinically indicated
Renal imaging every 1–3 years plus annual renal function tests
Chest HRCT every 5–10 years in adult women, more often if LAM detected
4. Management
Epilepsy: Infantile spasms – first-line vigabatrin; consider ACTH or steroids second-line. Drug‑resistant seizures: specialist neurologist referral, epilepsy surgery or ketogenic diet as appropriate.
SEGA: Monitor with MRI; surgical resection or mTOR inhibitor (everolimus) if large, growing or symptomatic.
Angiomyolipoma: mTOR inhibitors for lesions > 3 cm or bleeding; embolisation if bleeding; avoid nephrectomy if possible.
Pulmonary LAM (adult females): mTOR inhibitors; manage pneumothorax or lung transplant in advanced cases.
Skin lesions: Dermatology referral for topical/oral mTOR inhibitors, laser therapy, dermabrasion
Psychological/Behavioural: Multidisciplinary support – developmental pediatrics, psychiatry, psychology, behavioural therapy
Genetic counselling for patients and family members
Tuberous Sclerosis Cheat Sheet
| Domain | Summary |
|---|---|
| Genetics | Autosomal dominant (many sporadic); • TSC1 (chromosome 9) – hamartin • TSC2 (chromosome 16) – tuberin Adjacent to ADPKD1 → risk of renal cystic disease |
| Epidemiology | 1 in 5,000–10,000 births; ~50% have cognitive impairment; most have epilepsy |
| Pathology | Phakomatosis (neurocutaneous syndrome); multiple hamartomas in brain, skin, kidneys, retina, heart, lungs, liver, bone |
| History | Seizures, developmental delay, behavioural issues, family history, skin/cardiac/renal/lung involvement |
| Examination | Ash-leaf spots, facial angiofibromas, periungual fibromas, shagreen patch, retinal lesions, signs of LAM or AML |
| Differentials | • Neurofibromatosis Type 1 (NF1) • Von Hippel–Lindau (VHL) disease |
| Investigations | Brain MRI, renal US/MRI, ECG/Echo, Wood’s lamp, eye exam, genetic testing (TSC1/TSC2), HRCT |
| Management | Vigabatrin, mTOR inhibitors (SEGA, AML, LAM), epilepsy management, surgery, Multidisciplinary care and behavioural support |



























































{kind=link}
{kind=link}
{kind=link}