Consultations
Rheumatoid Arthritis
Rheumatoid Arthritis
History
HPC:
– Onset
– Progression
– Duration of Active symptoms/ current active symptoms
o Stiffness – duration of stiffness, morning or night
o Pain – pain worse morning or after exertion evening, any back or neck pain
o Weakness
o Warm
– Number of joints? Both sides? Legs and feet? Falls difficulty walking on uneven surfaces?
– What makes it worse? Cold weather pain change in colour?
– Ability to carry out ADL – shopping, dressing, cleaning, washing, cutlery use and cooking
– Dropping objects fine motor difficulties
– Rash
– Lumps on elbows or ankles? (Rheumatoid nodules)
– Weight loss, fevers, night sweats
– Chest pain sharp, breathlessness, cough (methotrexate pneumonitis)
– Numbness, loss of sensation in feet or fingers, burning pain, pins and needles
– Pain in neck or back, reduced range of motion, numbness and weakness in shoulders and arms.
– Polyuria, increased thirst, burning urine – blood sugars, haematuria
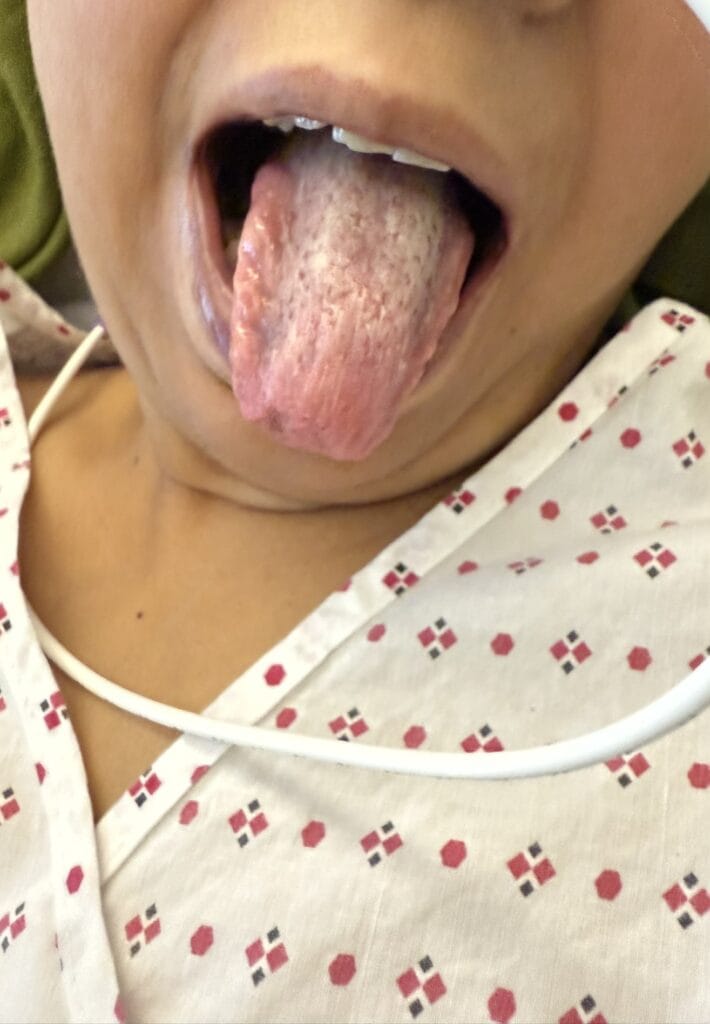
– Dry eyes, redness in eyes, pain in eyes. Mouth ulcers or genital ulcers?
– Difficulty swallowing – onset, progression, anything improve swallowing washing food down with fluid,
certain foods harder to swallow, hx of food sticking or regurgitation, heartburn water brash, Abdominal pain,
nausea, vomiting, perianal abscess, haematemesis? Diarrhea, bloating (small bowel malabsorption,
dysmotilitiy)
– Recent infections sore throat, fever, diarrhea? Any unwell contacts?
– Recent travel? TB endemic areas country of origin? TB contacts?
PMH:
Pregnancy or breast feeding
Previous joint surgery
MH:
– Analgesia use – NSAIDs – PPI with that – indigestion, black stools, nausea, swelling in ankles, blood
pressure
– DMARDs – side effects?
– Steroids injections or oral
– Bone protection – calcium vitamin d
– Biological therapies?
SH:
– Does condition interfere with employment, hobbies or home life?
– Occupation past – drilling vibrating tools?
– Smoking alcohol
– Adapted cutlery or aids for keys, writing, mobile phone?
– Physiotherapy input
FH:
Autoimmune conditions – HLA DR4 – extraarticular RA, SLE, Ankylosing Spondylitis, T1DM
HLAB27 – Enteropathic arthritis, Psoriatic Arthritis, Reactive Arthritis, Ankylosing Spondylitis
ICE
Examination
– Hand Examination and elbow inspection
o Temperature
o Radial pulse
o CRT
o Calcinosis
o Rheumatoid nodules elbows
– Inspection – flat on pillow and raised parallel to face
Z-thumb deformity
Boutonierres deformity
Swan neck deformity
Ulnar deviation
MCP subluxation
Inspect feet – fibular deviation, deformities, rheumatoid nodules achilles tendon
– Movements
o Pincer grip – make O don’t let me open it
o Power grip fingers
o Spread fingers like fan
o Make fist don’t let me bend your wrist
– Function
o Pick up coin, hold cutlery or cup
o Undo buttons
o Write with pen
o Brush hair
o Hands behind head – undo bra
– Sensation
o Radial
o Median
o Ulnar
o Phanel and Tinnel test
– Arms – elbows
o Rheumatoid nodules
o Calcinosis
o Measure blood pressure L+R (cervical rib)
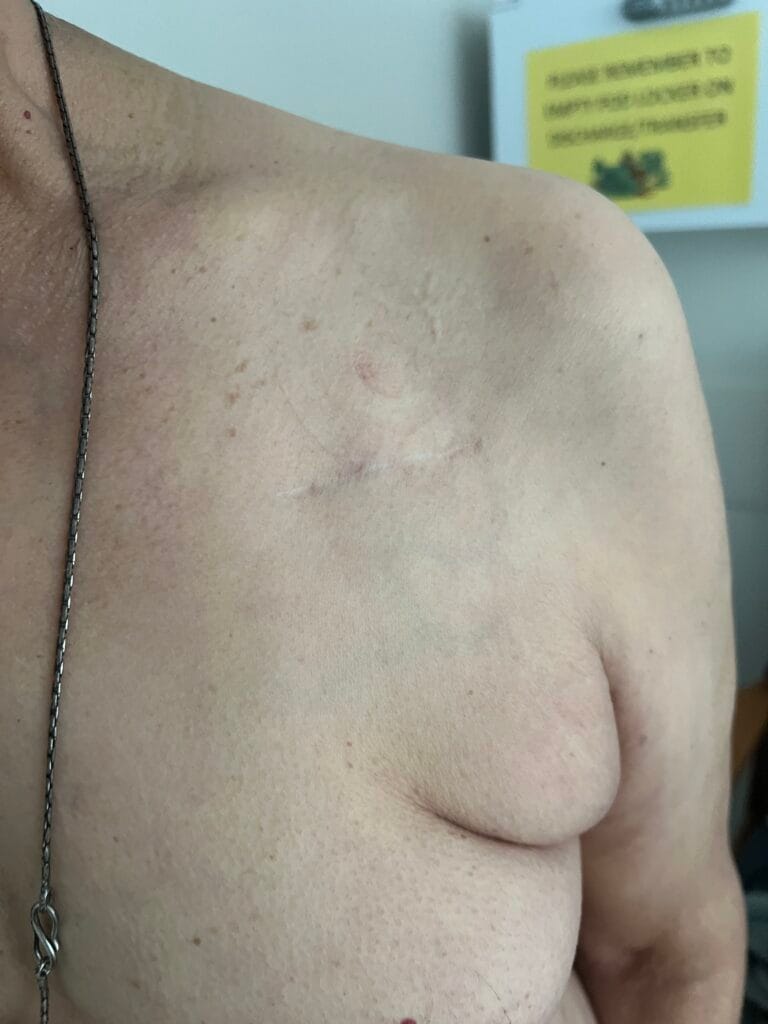
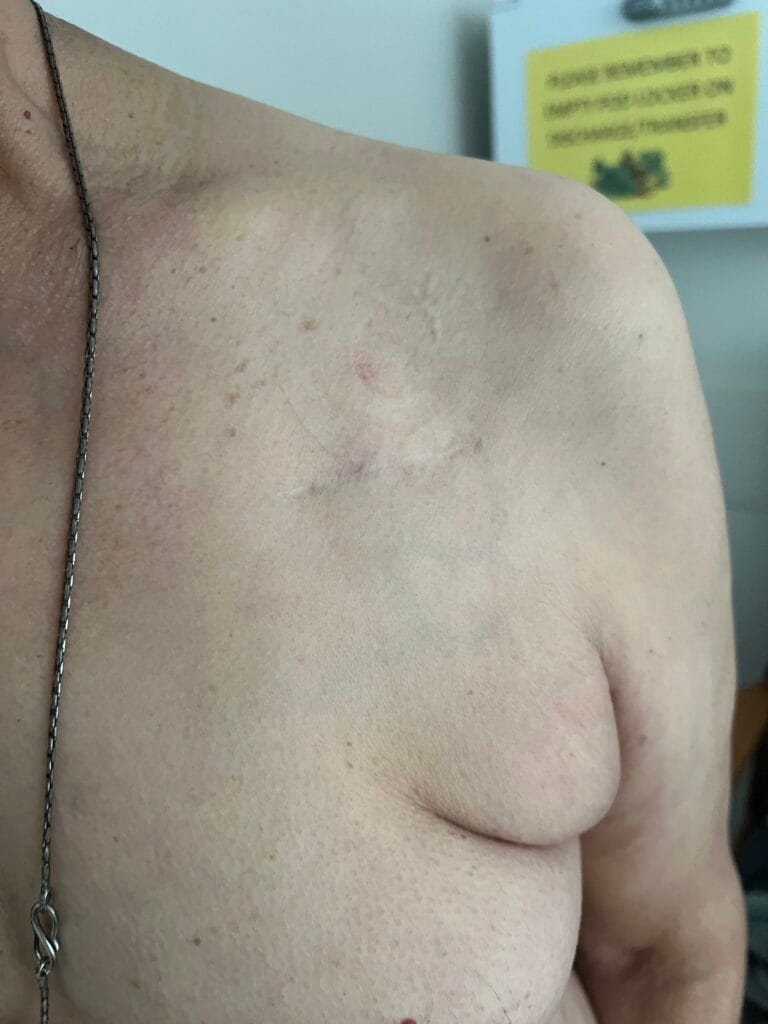
– Neck – scar atlantoaxial subluxation
o Range of movement
– Scalp and behind ears – psoriatic lesions
– Lower limb joint knee and ankle examination – feet fibular deviation
– Vasculitis – nailfold infarcts, scleritis, leg ulceration
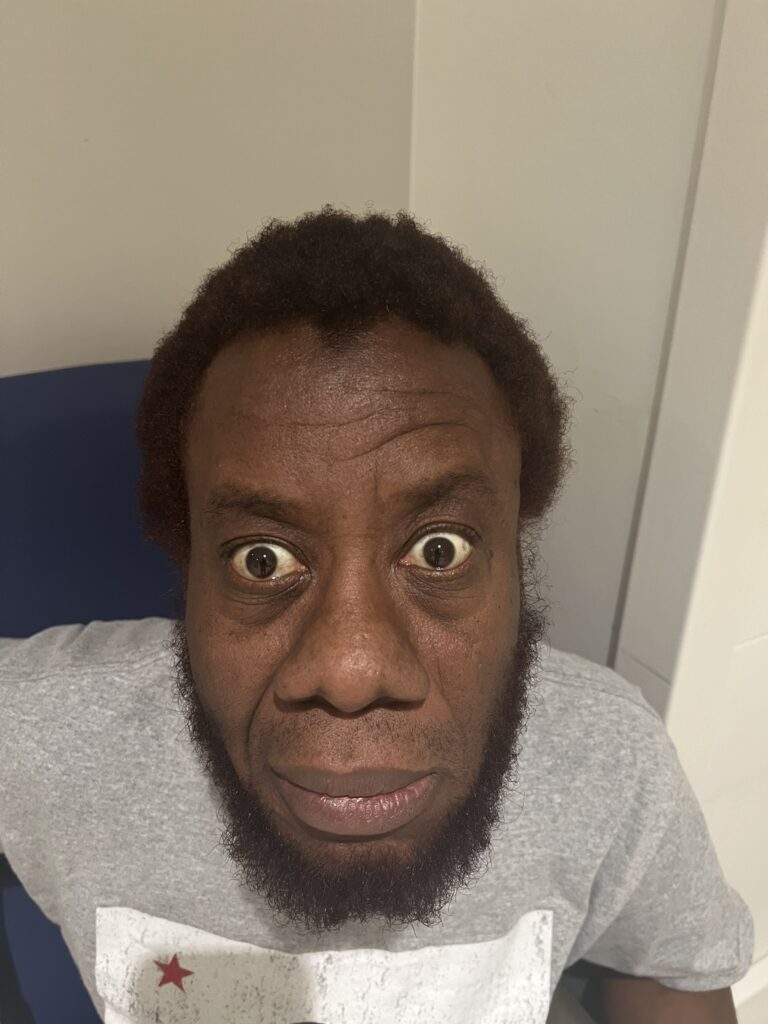
– Eyes
o Dry eyes, xerostomia
o Episcleritis, scleritis,
– Upper limb neuro – myelopathy from cervical spinal disease
– Lung Examination – auscultation
o Pleural effusion
o Interstitial lung disease
o Bronchiolitis obliterans
o Caplan syndrome
o Rheumatoid pulmonary nodules
– Abdominal
o Splenomegaly – feltys syndrome
– Cardiovascular
o Pulmonary hypertension
o ILD
Differential Diagnosis
– Psoriatic Arthropathy – scalp, postauricular, axillary, gluteal cleft erythematous well demarcated scaly lesions
– Systemic Lupus Erythematous – butterfly rash sparing nasolabial folds, scarring alopecia
– Polyarticular gout – classically MTP joint, risk factors – diuretics, diet, alcohol
– Seronegative arthropathies – Ankylosing spondylitis, Reactive Arthritis
– Nodal OA
Investigations
I would like to order:
– Blood tests including FBC to check for anaemia secondary to
o Chronic disease
o Felty’s syndrome splenomegaly
o Methotrexate use causing myelosuppression
o GI bleeding 2ry to NSAID use
§ ESR
§ CRP
§ U+Es
§ LFTs
§ Rheumatological specific blood tests: Rheumatoid factor, anti-CCP
§ Sclerosis – ANA, Anti-centromere, Anti-scl, immunoglobulins, anti-RNA polymerase
§ SLE – C3/C4 complements reduced, Anti-dsDNA, ENA
– Urinalysis – check for proteinuria or haematuria secondary to
o Renal vasculitis, amyloidosis, urine infections (myelosuppression), interstitial nephritis NSAIDs
– X-ray of hands and feet
o Reduce joint space
o Periarticular erosions and osteopenia
– CXR – to check for interstitial lung disease or pleural effusions + Pulmonary Function Tests
– MRI of cervical spine if signs of myelopathy
– Nerve conduction studies if possible carpal tunnel syndrome
Management
– Patient information, education and support groups
– Referral to rhematology OT CNS
– Hospital leaflets and Arthritis Research Council
– Occupational therapy: splints, adjusted cutlery with large handles, adjusted key grips, jar grips and sticks to
pick up things off floor. Community team household improvements bath seats, rails in shower
– Physiotherapy – strengthening of muscles and preserve joint function
– Analgesia
– Bone protection if on steroids / consider DEXA if any previous fractures.
– DMARDs
o Methotrexate (contraindicated if pregnancy), sulphasalazine, hydroxychloroquine, leflunomide
o Failed DMARDs or persistent disease
§ Anti-tnf – infliximab, adalimumab, entanercept
§ Anti CD 20 – rituximab
§ Anti-IL6 – tocilizumab
JAK 2 inhibitors
– Surgical
o Arthoplasty
o Arthrodesis
o Synovectomy
Medication side effects
Methotrexate – hepatitis, cytopenia, pneumonitis, ILD – FBC, LFTs every 2 weeks then 1-3months
– Men taking methotrexate – 3 month washout period before trying to conceive
– Women of childbearing age birth control 6 months washout period. Avoid while breastfeeding and wait 1
week after terminating before breastfeeding.
Hydroxychloroquine – visual disturbance, retinopathy – check baseline acuity and annually thereafter
Sulphasalazine – hepatitis, rash, discolouration sweat/urine – FBC and LFTs every 2 weeks 3/12 then 3/12
Leflunomide – hepatitis, myelosuppression, rash – FBC and LFTs every 2 weeks then 2/12
Gold – rash, eosoniphilia, cytopenia – FBC, and urinalysis before each injection
Corticosteroids – weight gain, bruising, fluid retention, diabetes, osteoporosis, cataract, glaucoma– bone
density measurement and bone protection all patients >3 months
Azathiorpine – cytopenia, oncogenicity – FBC and LFTs every 2 weeks then 3/12
Ciclosporin – renal impairment and hypertension – FBC, serum creatinine level and blood pressure weekly
then ever month
Cyclophosphamide – interstitial nephritis, hemorrhagic cystitis – FBC and urinalysis monthly
RA sparing DIP joints // Psoriatic arthropathy asymmetric oligoarthritis involving distal DIP joints with less than
5 small/large joints (hands and feet initially), arthritis mutilans – telescoping, sypondyloarthritis (sacroiliitis and
spondylitis). Hyperkeratosis of nail plates.
Psoriasis = Erythematous well demarcated plaques distributed over extensor prominence, trunk and scal and
intragluteal cleft. Plaques are circular with well defined edges and a livery scale. Pitting of fingernails and
onycholysis with some of the nail plates thickened with thick scale resembling hyperkeratosis.
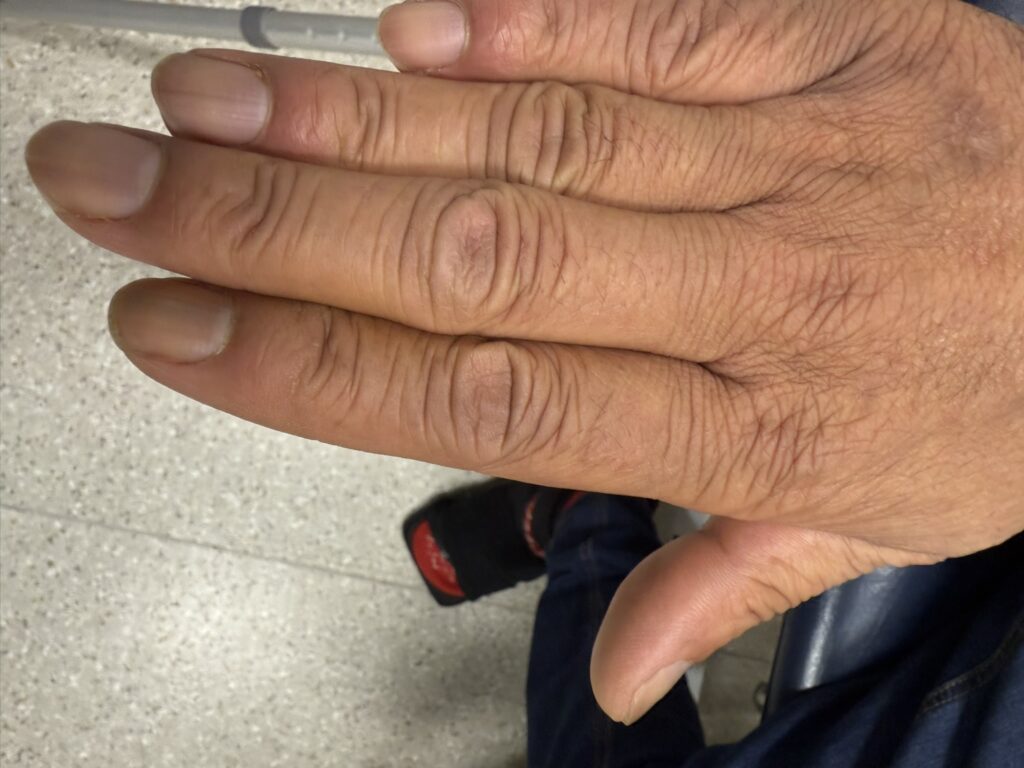
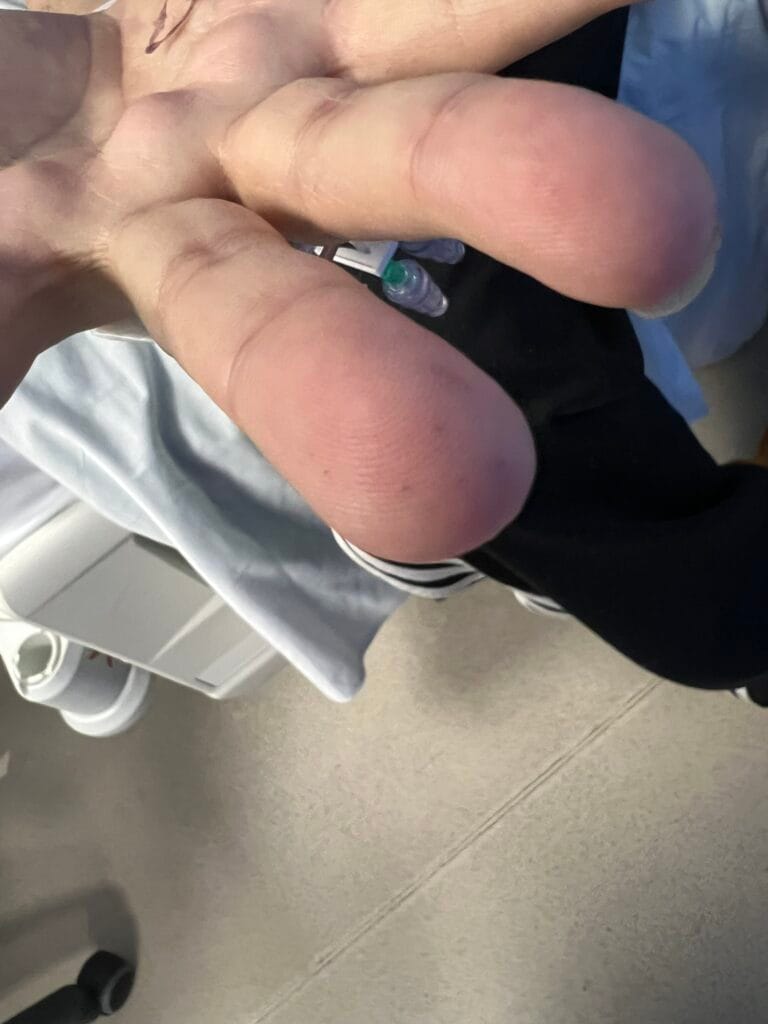
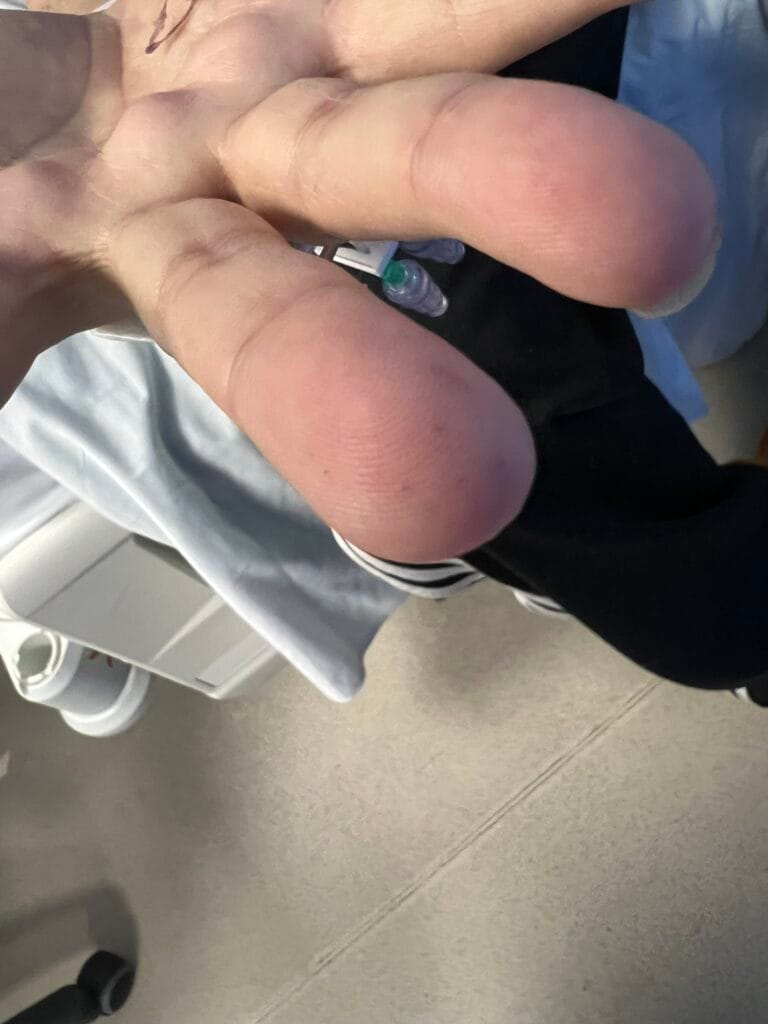
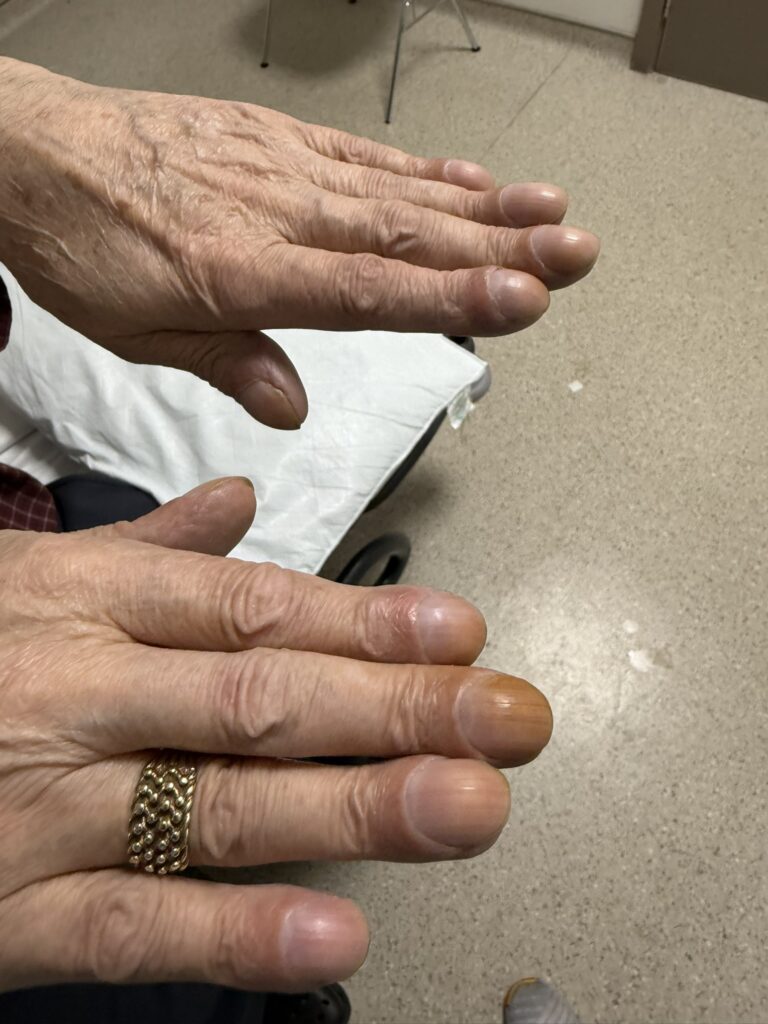
RA = Symmetrical deforming polyarthropathy predominantly affecting small joints of hands with spindling of
fingers due to soft tissue swelling at PIP and MCP joints. DIP joints are spared. There is generalized wasting
of small muscles of hands and use is restricted by weakness, deformity and pain. Nodules at elbow over
extensor tendons and in the palm. There is ulnar deviation of the fingers (consequent upon subluxation and
dislocation of MCP joints). Prescence of warmth, pain and swelling suggests active inflammation at present.
This patient has RA.
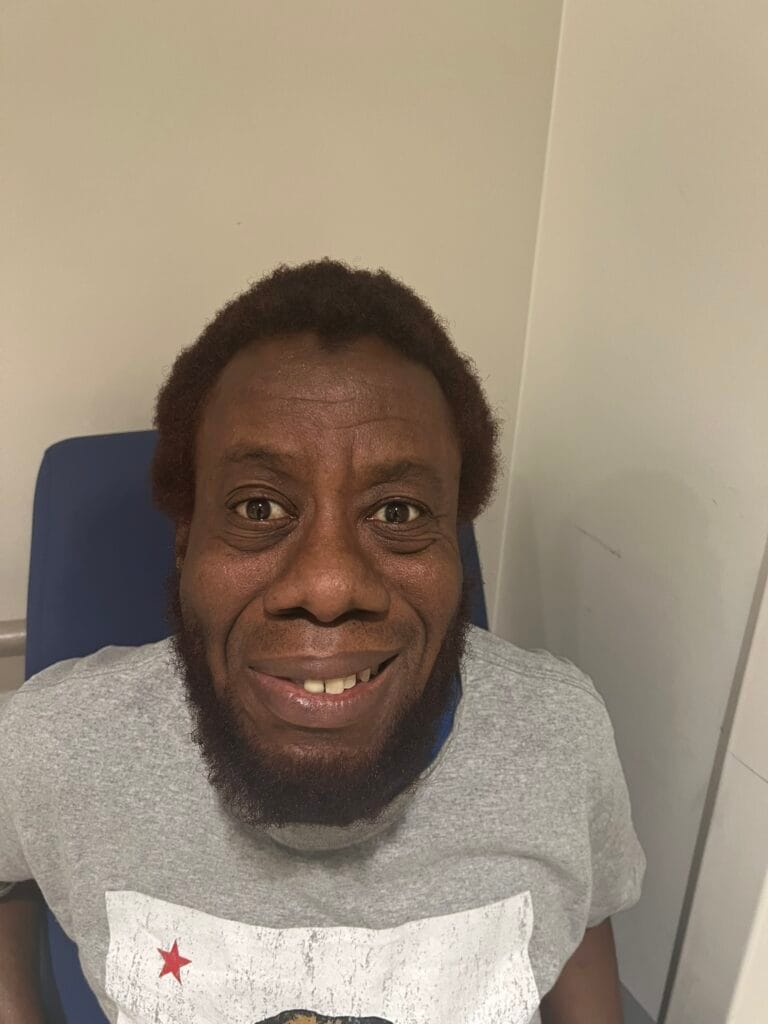
Systemic Sclerosis = This patient displays microstomia, telangiectasia, sclerodactyly, nailfold capillary
dilatation, atrophy of finger tips and digital ulceration. Clinical signs of CREST syndrome