Consultations
Diabetic Retinopathy
In Station 5 you may be asked to assess a diabetic patient who has concerns about their vision.
Station Instructions: This 52-year-old man with type 2 diabetes has noticed that his vision has become blurred and is worried about going blind. Please assess him.
1. Key History-Taking Points
Visual Symptoms
- Character of blurring: near, far, or all distances? Blurred even with glasses or contact lenses? Any change in prescription recently?
- Timing: since when, sudden vs gradual onset, constant vs intermittent, getting worse, previous episodes
- Laterality: one or both eyes
- Painful or painless (painful = glaucoma, scleritis, uveitis; painless = most retinal causes)
- Loss of vision: any missing patches, field loss, bumping into things
- Double vision (cranial nerve palsy — diabetic mononeuritis multiplex)
- Floaters, dark spots, flashers: vitreous haemorrhage, retinal detachment
- Halos or glare: cataracts, glaucoma
- Impact on daily life
- Driving: does the patient drive, and what type of licence — Group 1 (car) or Group 2 (lorry/bus)?
Diabetic History
- Diagnosis: when diagnosed, Type 1 or Type 2
- Treatment and compliance: diet, oral hypoglycaemics, insulin; any recent changes
- Glycaemic control: home blood sugar readings, target range, most recent HbA1c
- Hospital admissions: diabetic ketoacidosis, hyperosmolar states, severe hypoglycaemia
- Eye history: previous retinopathy, attendance at diabetic eye screening, laser treatment, seen by ophthalmologist
- Renal: known proteinuria, CKD, dialysis (renal involvement correlates with retinopathy severity)
- Blood pressure: known hypertension, current treatment (hypertension accelerates retinopathy)
- Hypoglycaemia: frequency, severity, awareness
- Neuropathy: pins and needles, numbness, bladder dysfunction, erectile dysfunction, falls
- Feet: ulcers, claudication, pulse problems
- Cardiovascular: MI, stroke, angina; full CVS risk factor history (smoking, hypercholesterolaemia)
2. Key Examination Findings
Visual Acuity
- Test each eye separately, with and without glasses/contact lenses
- Use Snellen chart; document result (e.g. 6/12, 6/6)
- Pinhole to distinguish refractive error from pathology
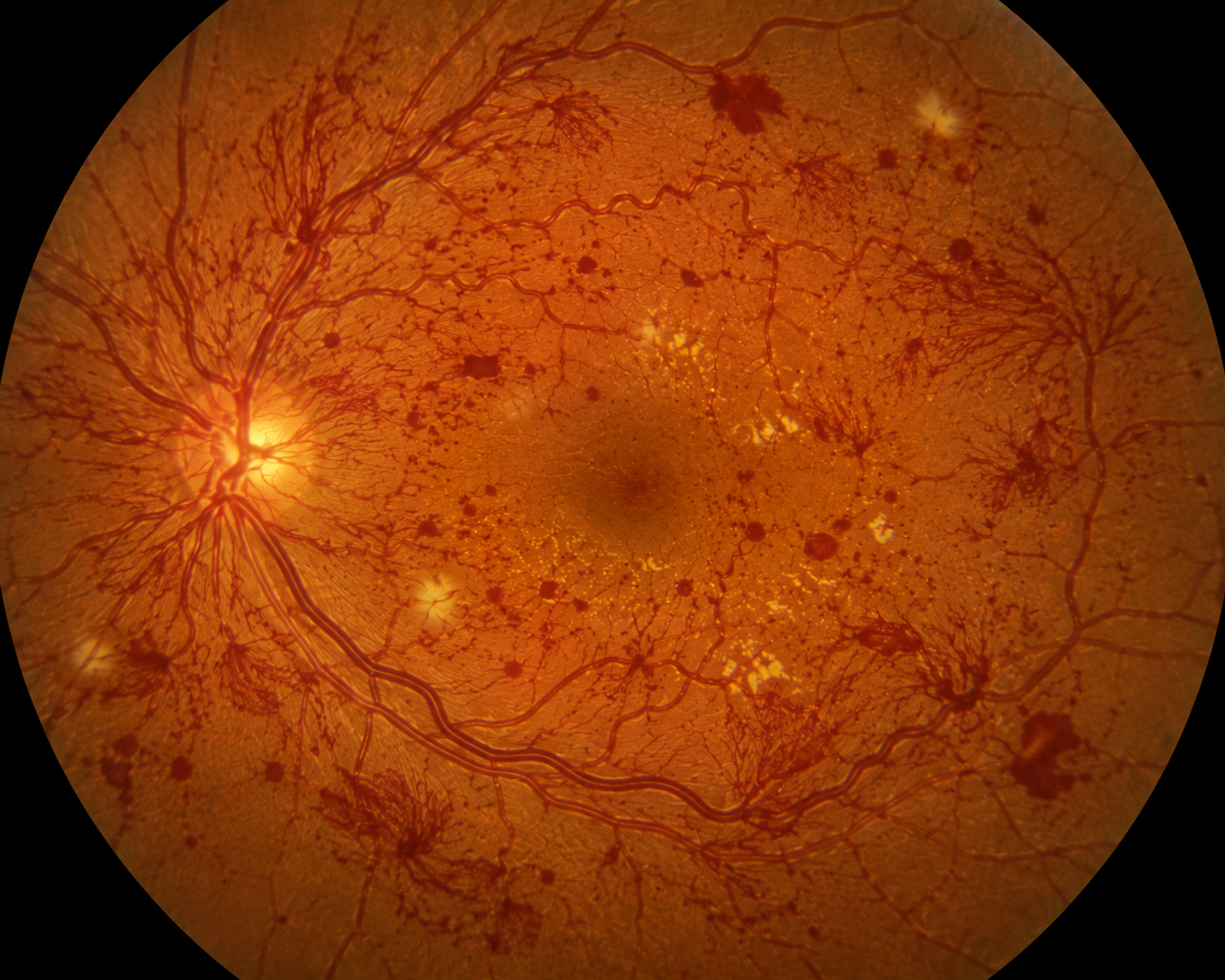
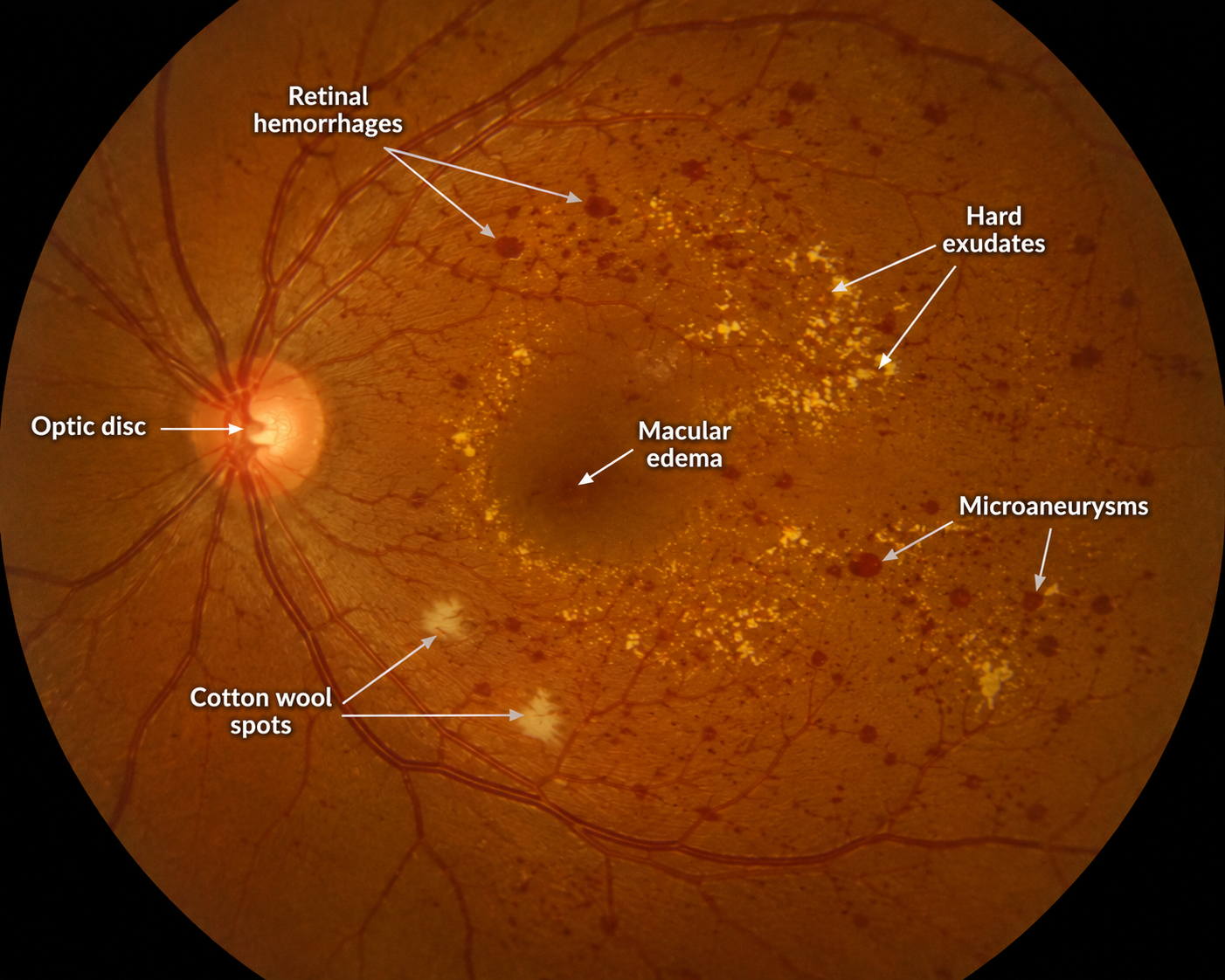
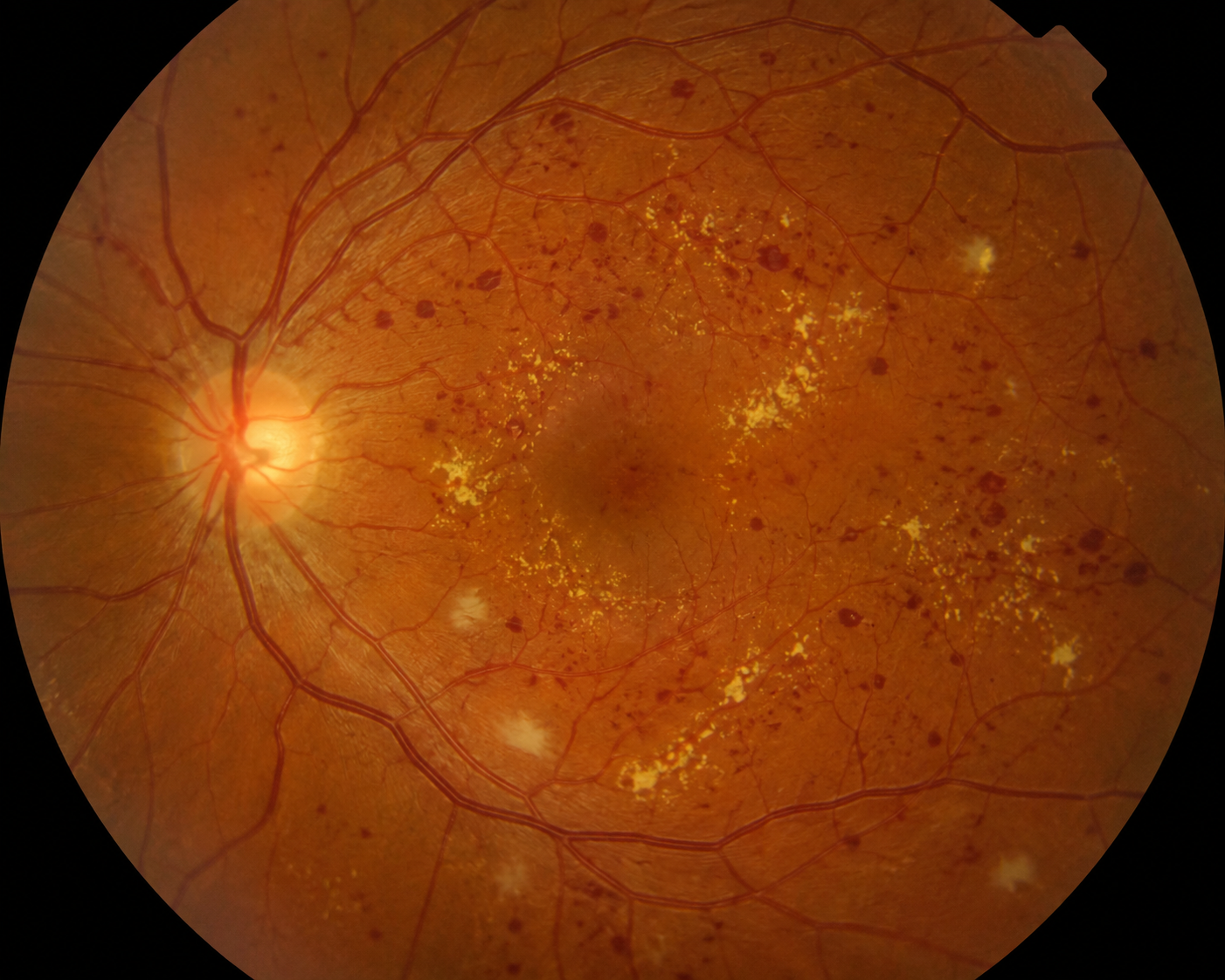
Fundoscopy — What to Look For
- Background (mild non-proliferative) DR: microaneurysms (dots), dot and blot haemorrhages, hard exudates
- Moderate non-proliferative DR: more haemorrhages and exudates, cotton wool spots (nerve fibre layer infarcts), venous beading
- Severe non-proliferative DR: extensive blot haemorrhages in all four quadrants, venous beading and looping, intraretinal microvascular abnormalities (IRMA) — the 4-2-1 rule
- Proliferative DR: new vessel formation at the disc (NVD) or elsewhere on the retina (NVE) — high risk of vitreous haemorrhage and traction retinal detachment
- Maculopathy: hard exudates or haemorrhages within one disc diameter of the fovea, or thickening of the macula (macular oedema) — most common cause of visual loss in diabetic patients
Additional Examination
- Visual fields: if time allows
- Eye movements and pupils: cranial nerve palsies (CN III, IV, VI — mononeuritis multiplex)
- Blood pressure: offer to measure; hypertension accelerates retinopathy
- Capillary blood glucose: offer to check today
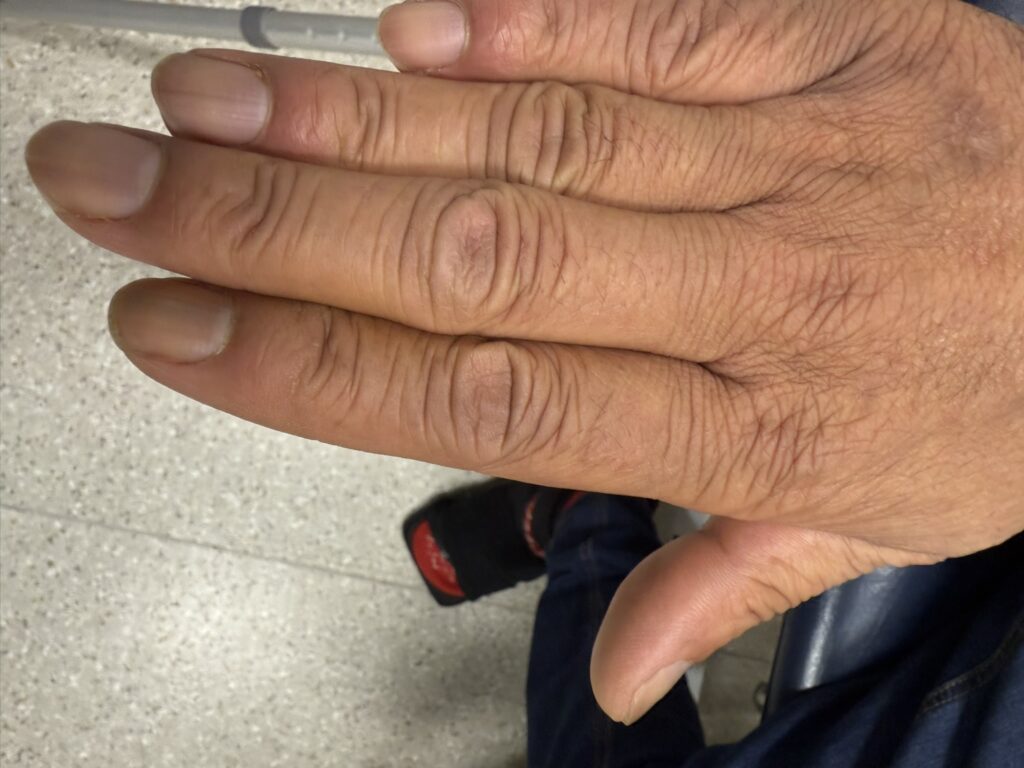
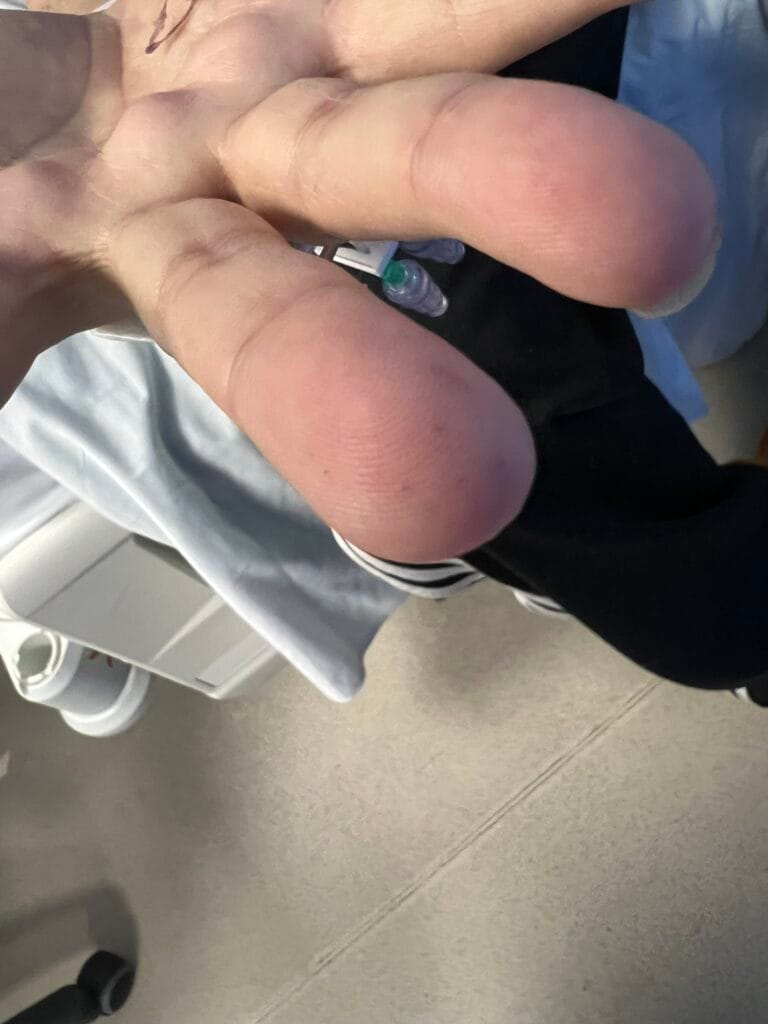
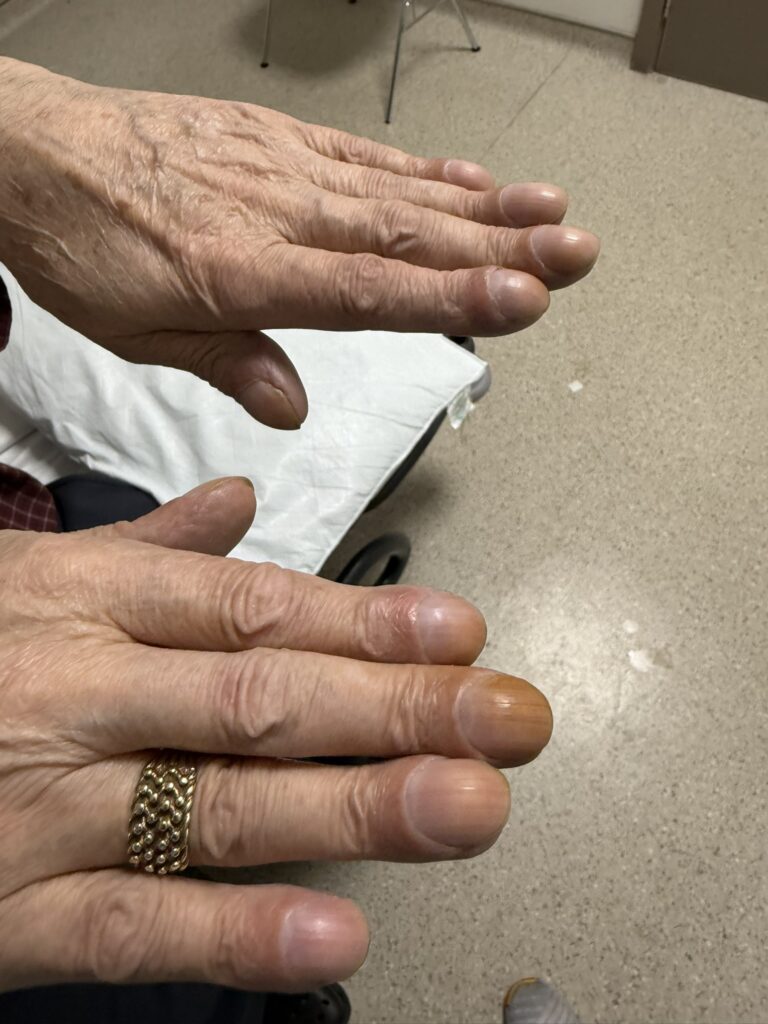
- Diabetic fingerprick marks on fingertips
- Feet examination: peripheral neuropathy (monofilament, vibration sense, ankle jerks), ulcers, peripheral pulses
- Quick cardiovascular assessment if time allows
Model Explanation template: “The retina is a light-sensitive layer at the back of your eye. Persistently high blood sugar damages the tiny blood vessels that supply it — they weaken, bleed, leak fluid and can become blocked. The retina then tries to grow new blood vessels, but these are fragile and tend to bleed, which can threaten your sight. The good news is that laser treatment can seal these new vessels and greatly reduce the risk of serious vision loss. I would like to refer you to an eye specialist today who has better equipment to assess this in detail. In the meantime, I would like to check your blood sugar and HbA1c today, and also check your blood pressure, cholesterol and kidney function. Improving blood sugar control and blood pressure can significantly slow any further damage. I would also advise you not to drive until you have been seen by the eye doctor.”
3. Specific Investigations
Bloods
- HbA1c: degree of glycaemic control over preceding 3 months
- Fasting glucose
- Fasting lipid profile
- U&E and eGFR: renal involvement (nephropathy correlates with retinopathy)
- FBC
Urine
- Urine dipstick: proteinuria, haematuria
- Urine albumin:creatinine ratio (ACR): microalbuminuria (early nephropathy)
Other
- Blood pressure measurement
- ECG
- Ophthalmology referral for slit-lamp biomicroscopy and formal fundus assessment with dilated pupils — better than direct ophthalmoscopy for macular detail
- Optical coherence tomography (OCT) — detects and quantifies macular oedema
- Fluorescein angiography — maps retinal vascular leakage and new vessels
4. Management
Optimise Systemic Risk Factors
- Glycaemic control: tighten HbA1c to target; refer to diabetic specialist nurse; adjust medications or initiate insulin if required
- Blood pressure: target <130/80 mmHg in diabetic patients with retinopathy; ACE inhibitors or ARBs preferred (renoprotective)
- Lipids: statin therapy to reduce cardiovascular and microvascular risk
- Lifestyle: smoking cessation, weight loss, exercise
Ophthalmology Referral & Thresholds
- Routine ophthalmology referral: moderate non-proliferative DR
- Urgent referral (routine ophthalmology): maculopathy, severe non-proliferative DR
- Urgent 2-week referral: proliferative diabetic retinopathy
- Emergency same-day referral: vitreous haemorrhage, tractional retinal detachment, sudden severe visual loss
Ophthalmic Treatment
- Laser photocoagulation (pan-retinal photocoagulation): treatment of choice for proliferative DR — destroys ischaemic peripheral retina to regress new vessels
- Focal/grid laser: for clinically significant macular oedema
- Intravitreal anti-VEGF injections (e.g. ranibizumab, aflibercept): first-line for centre-involving diabetic macular oedema; also used in proliferative DR
- Intravitreal steroid implants (e.g. dexamethasone implant): for refractory macular oedema
- Vitrectomy: for vitreous haemorrhage, tractional retinal detachment
Driving Advice
- Advise patient not to drive until assessed by ophthalmology
- Must notify DVLA if: laser treatment needed; problems with vision in both eyes; impaired hypoglycaemia awareness; >1 severe hypoglycaemic episode in last 12 months (or any single episode for Group 2 drivers); insulin treatment; leg/foot problems requiring automatic vehicles only; tablet treatment (Group 2 drivers)
- Group 1 (car/motorcycle): visual acuity ≥6/12 both eyes together; field of vision ≥120° horizontal; able to read a number plate at 20 metres
- Group 2 (lorry/bus): ≥6/7.5 best eye; ≥6/60 other eye; field of vision ≥160° horizontal
Diabetic Retinopathy Cheat Sheet
| Domain | Summary |
|---|---|
| Stages of DR |
Background (mild non-proliferative): microaneurysms, dot and blot haemorrhages, hard exudates Moderate non-proliferative: more haemorrhages/exudates, cotton wool spots, venous beading Severe non-proliferative (4-2-1 rule): blot haemorrhages all 4 quadrants, venous beading ≥2 quadrants, IRMA ≥1 quadrant Proliferative: new vessels at disc (NVD) or elsewhere (NVE) — risk of vitreous haemorrhage and traction retinal detachment Maculopathy: exudates/haemorrhages within 1 disc diameter of fovea; macular oedema — most common cause of visual loss |
| Pathophysiology | Chronic hyperglycaemia → pericyte loss, BM thickening → microaneurysm formation → haemorrhage, exudate, capillary occlusion → retinal ischaemia → VEGF release → neovascularisation → vitreous haemorrhage / tractional detachment |
| Risk Factors for Progression | Poor glycaemic control (HbA1c), hypertension, nephropathy, hyperlipidaemia, duration of diabetes, pregnancy, smoking, anaemia |
| Fundoscopy Findings | Microaneurysms (dots), blot haemorrhages, hard exudates (lipid), cotton wool spots (nerve fibre infarcts), venous beading/looping, IRMA, NVD/NVE, macular oedema, vitreous haemorrhage (loss of fundal view) |
| Referral Thresholds | Routine: moderate NPDR. Urgent (routine ophthalmology): maculopathy, severe NPDR. 2-week referral: proliferative DR. Same-day emergency: vitreous haemorrhage, tractional RD, sudden visual loss |
| Treatment | Pan-retinal laser photocoagulation (proliferative DR); focal/grid laser (macular oedema); anti-VEGF intravitreal injections (macular oedema, proliferative DR); dexamethasone implant (refractory macular oedema); vitrectomy (vitreous haemorrhage, tractional RD) |
| Other Visual Problems in Diabetes | Maculopathy, vitreous haemorrhage, retinal detachment, CRAO/BRAO, CRVO/BRVO, stroke/TIA, ischaemic optic neuropathy, glaucoma, cataract, ocular muscle palsies (CN III, IV, VI mononeuritis multiplex) |
| Differentials of Visual Disturbance | Diabetic retinopathy, retinal detachment, macular degeneration, migraine with aura, TIA/stroke, postural hypotension, hypoglycaemia |
| DVLA & Driving | Group 1: VA ≥6/12 both eyes, field ≥120° horizontal. Group 2: ≥6/7.5 best eye, ≥6/60 other, field ≥160°. Must notify DVLA: laser treatment, bilateral visual problems, impaired hypo awareness, >1 severe hypo/12 months (1 episode Group 2), insulin use, tablet use (Group 2), limb problems requiring automatic vehicle |
☐