
Dermatomyositis
Dermatomyositis is an autoimmune inflammatory myopathy characterized by symmetrical proximal myopathy and distinctive photosensitive skin rashes such as the heliotrope rash and Gottron papules. It is often assosciated with interstitial lung disease, dysphagia and an increased risk of underlying malignancy.
Station Instructions: Assess this patient presenting with a rash and weight loss.1. Key History‑Taking Points
History of Presenting Complaint:
Muscle Symptoms
Weakness: Onset, duration, and pattern (symmetrical proximal limb weakness — difficulty climbing stairs, combing hair, rising from chair).
Pain: Myalgia or tenderness?
Fatigue: Associated with exertion?
Progression: Rate of worsening, any swallowing or breathing difficulty (bulbar or respiratory involvement).
Skin Symptoms
Rash:
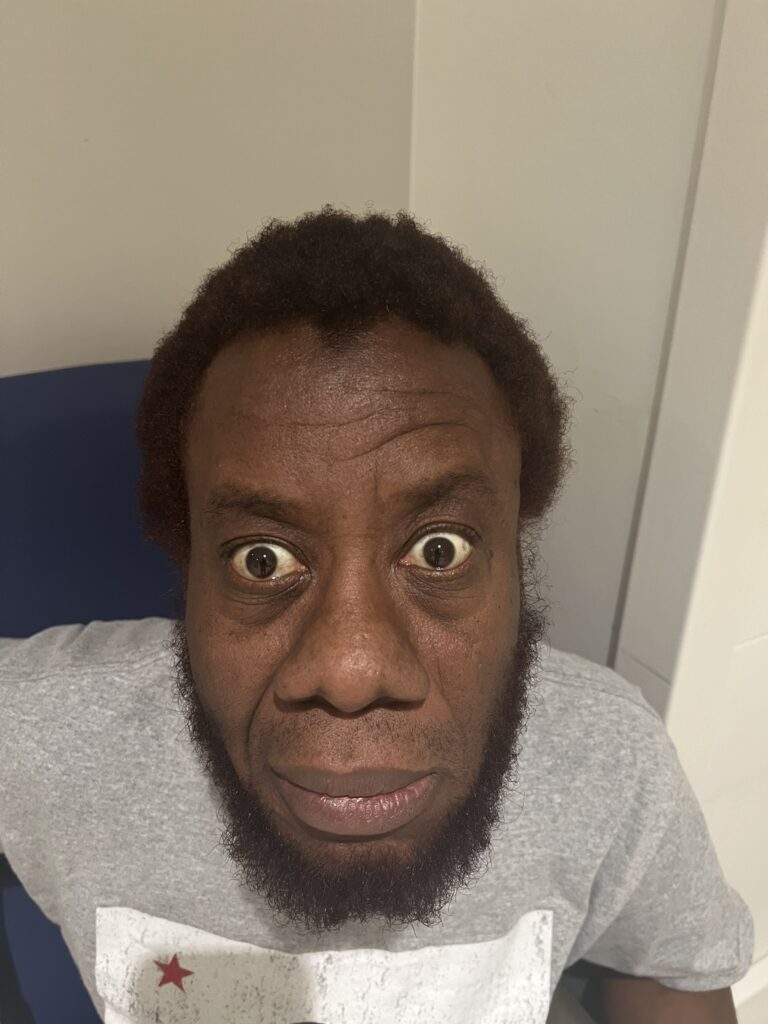
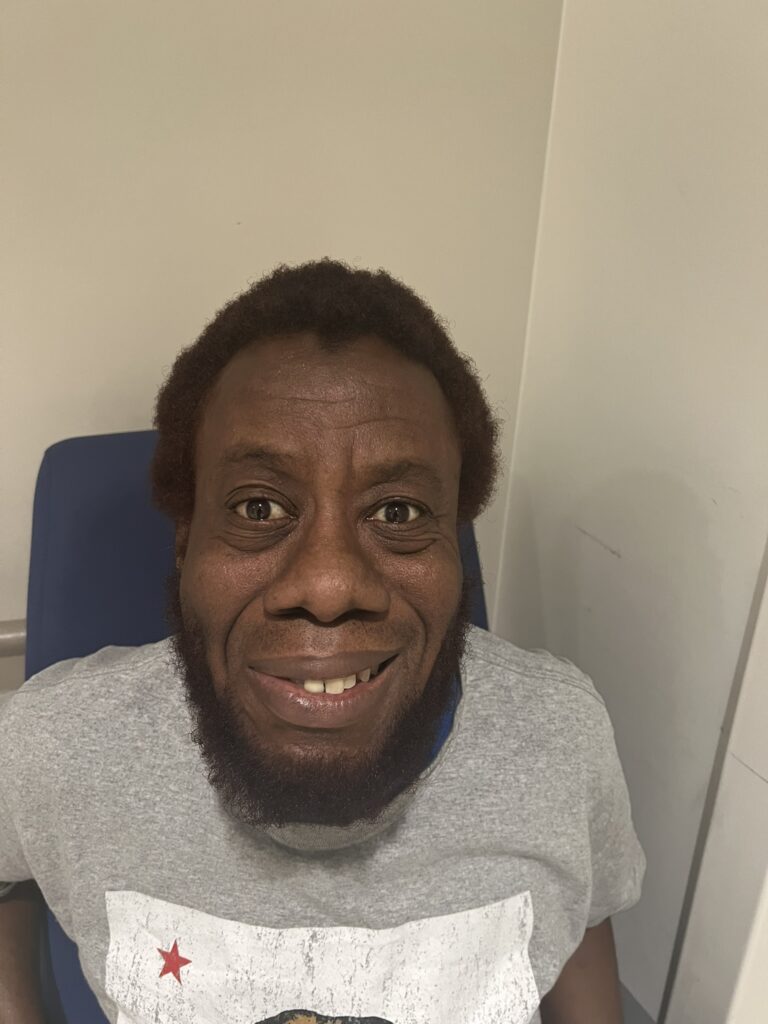
Heliotrope rash (violaceous periorbital discolouration, eyelid oedema)
Gottron’s papules (scaly papules over MCP, PIP joints)
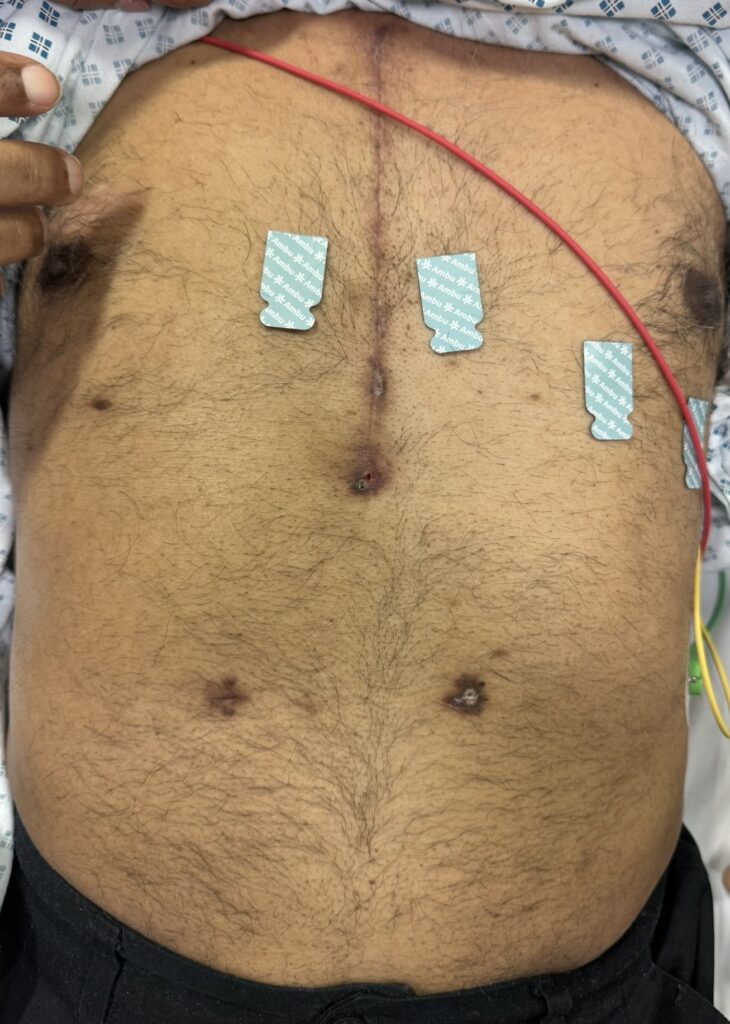
Shawl sign (photosensitive rash over shoulders, neck, upper chest)
V-sign (anterior chest rash)
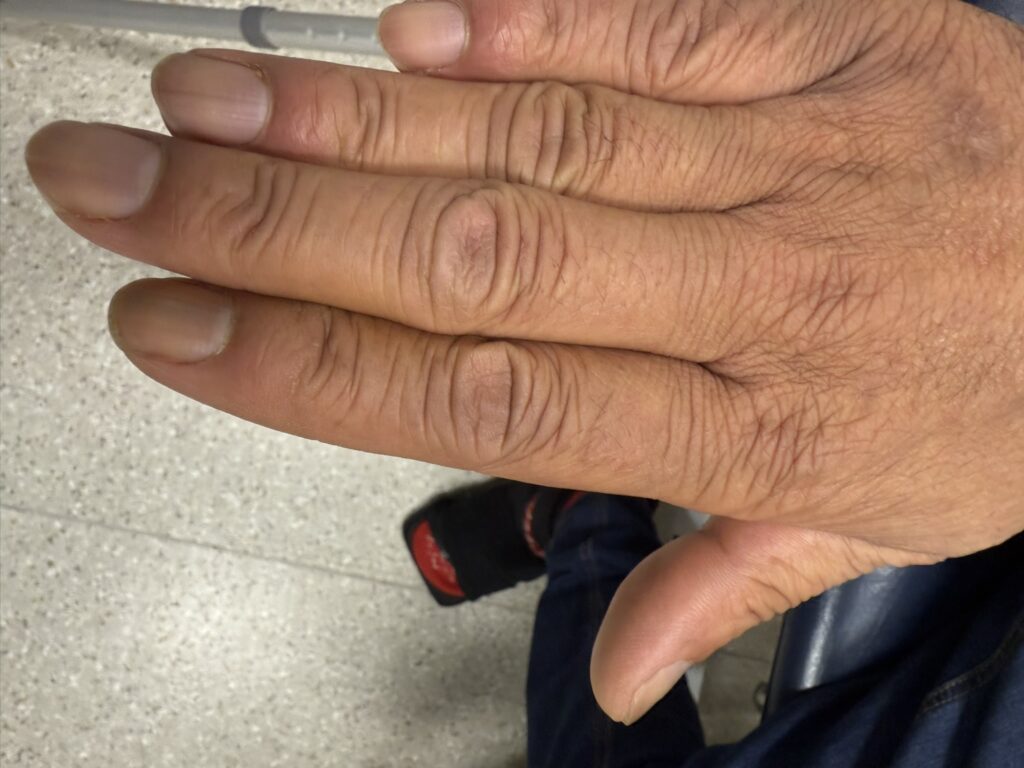
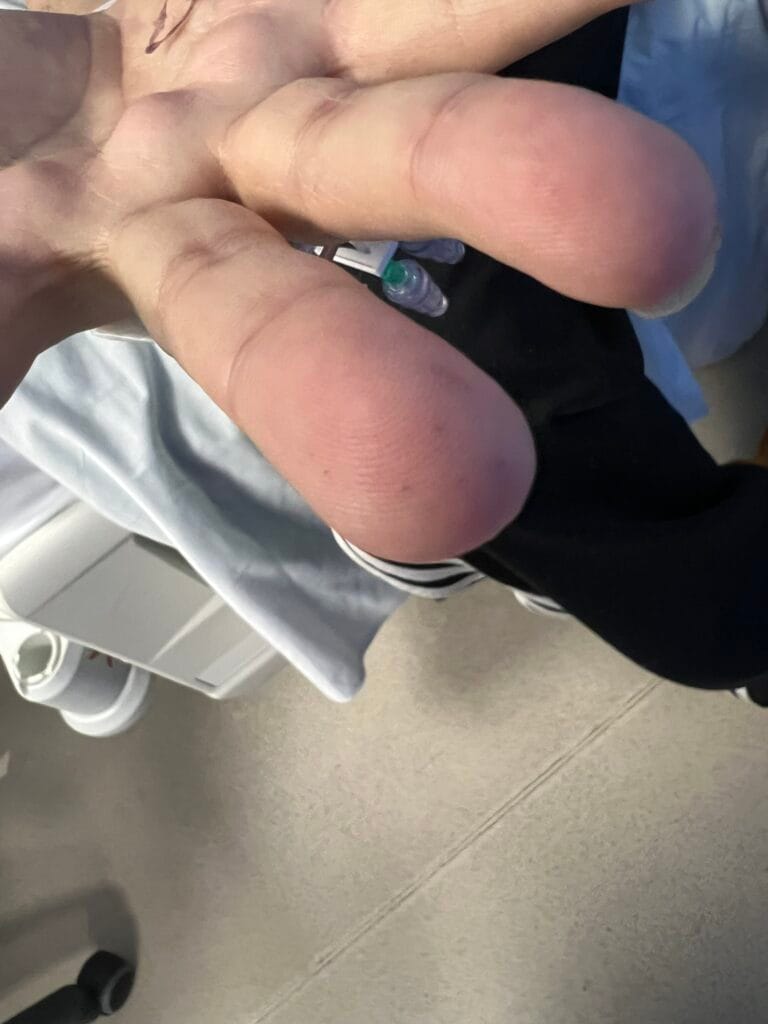
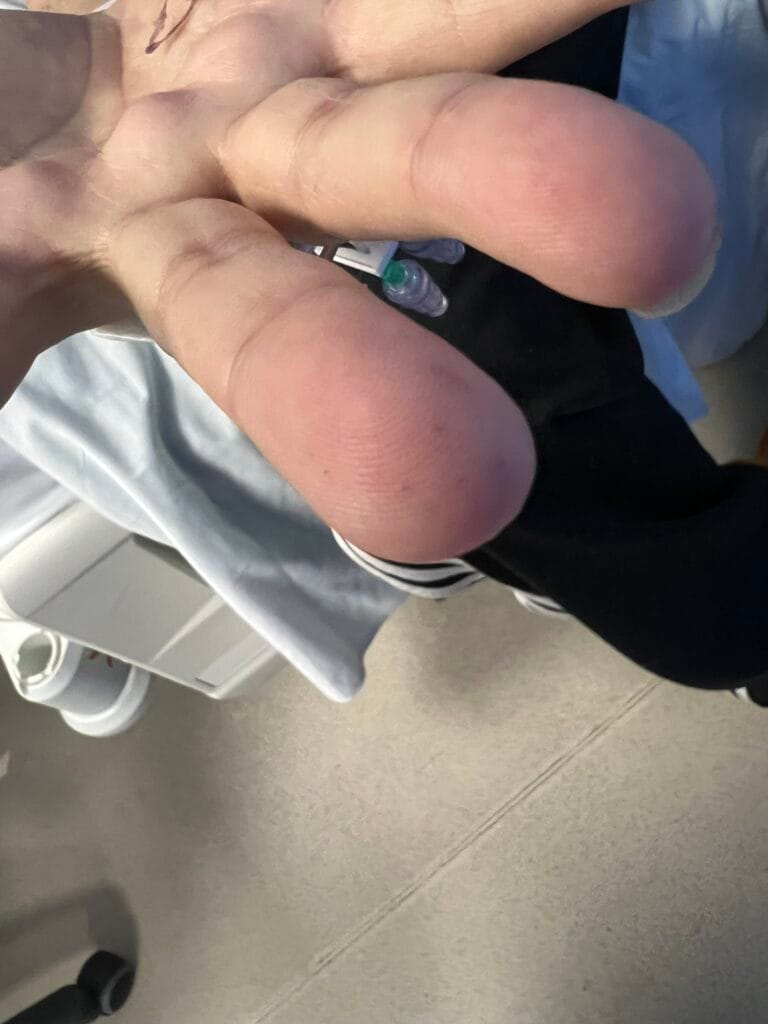
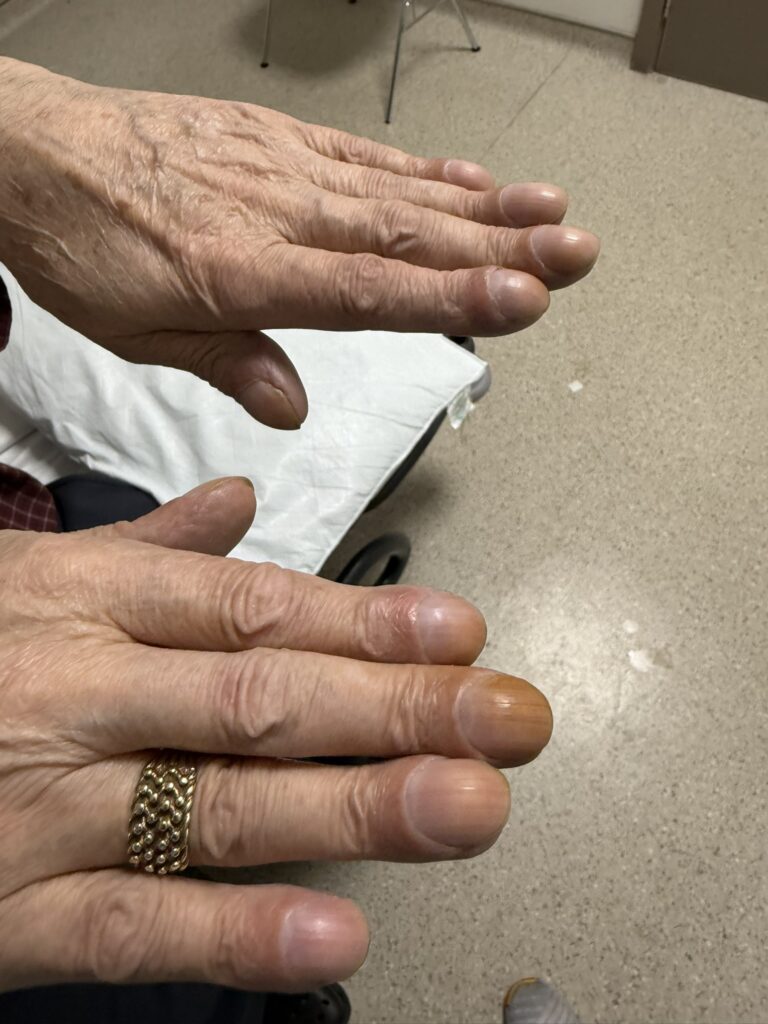
Mechanic’s hands (hyperkeratotic fissuring on lateral fingers)
Photosensitivity
- Nail Changes: periungual erythema (redness), ragged cuticles, longitudinal ridging, dilated nailfold capillaries and splinter haemorrhages
Systemic Symptoms
Respiratory: Cough, breathlessness (interstitial lung disease)
Dysphagia / dysphonia: Oesophageal or pharyngeal weakness
Constitutional: Weight loss, fever, fatigue
Arthralgia: Overlap with other connective tissue diseases
Malignancy Screening History (age and gender-specific malignancy screening)
Weight loss, night sweats, postmenopausal bleeding, haematuria, cough, breast changes, bowel symptoms
Previous malignancy, family history of cancer
Past Medical & Family History
Other autoimmune diseases (SLE, scleroderma, RA, thyroid disease)
Family history of myositis or connective tissue disease
Drug & Exposure History
Drugs: statins, hydroxyurea, penicillamine
UV exposure, recent infection, or vaccination
Functional Impact
Difficulty performing daily tasks, occupation impact, fatigue, emotional wellbeing
2. Key Examination Findings
General Inspection:
Periorbital violaceous rash (heliotrope rash)
Gottron’s papules over MCP joints, knees or elbows
Shawl or V-sign rash on chest and upper back
Mechanic’s hands (rough, fissured skin on fingers)
Raynaud’s phenomenon
Nail changes: Periungual erythema, dilated capillaries, ragged cuticles, longitudinal ridging, splinter haemorrhages
Muscle Examination:
Symmetrical proximal muscle weakness (shoulder and hip girdle)
Muscle tenderness, wasting (late stage)
Assess tone, reflexes (usually normal)
Test bulbar and neck flexor strength
Systemic Examination:
Respiratory: fine bibasal end-inspiratory crackles (ILD)
Cardiovascular: arrhythmias, cardiomyopathy
Abdominal: organomegaly or masses (malignancy)
3. Specific Investigations
Blood Tests:
↑ Muscle enzymes: CK, aldolase, AST, ALT, LDH
Autoantibodies:
Myositis-specific: anti-Mi-2, anti-MDA5, anti-TIF1-γ, anti-NXP2
Myositis-associated: anti-Jo-1, anti-PL-7, anti-PL-12 (antisynthetase syndrome)
ANA, ENA screen
FBC, U&E, ESR, CRP
Imaging & Functional Tests:
MRI of muscles: oedema and inflammation
EMG: myopathic pattern (short, low-amplitude potentials)
Muscle biopsy: perivascular and perifascicular inflammation, fibre necrosis (diagnostic)
Malignancy Screening:
Age and gender-appropriate screening (urinalysis, PSA, mammogram, pelvic/trasnvaginal ultrasound, colonoscopy, CT chest/abdomen/pelvis)
PET-CT if paraneoplastic suspicion
Other Tests:
Pulmonary function tests ± HRCT for interstitial lung disease
Echocardiogram if cardiac involvement suspected
Capillaroscopy of nailfoldes (dilated capillaries)
Skin biopsy (interface dermatitis)
4. Differentials
- SLE
- Scleroderma
- Sjogren’s Syndrome
- Inflammatory Myopathis (Polymyositis, drug-induced myopathies)
5. Management
Multidisciplinary Approach:
Dermatology, Rheumatology, Neurology, Oncology, Respiratory, Physiotherapy
General Measures
- Rest during acute phase, then graded physiotherapy
- Sun protection and topical emollients for rash
Psychological and occupational support
Pharmacological Treatment
- Corticosteroids: Oral prednisolone (1 mg/kg/day), slow taper
- Steroid-sparing agents: Methotrexate, azathioprine, mycophenolate, or cyclophosphamide (if resistant)
- IV immunoglobulin (IVIG): for refractory or severe disease (esp. dysphagia)
- Biologics: Rituximab or JAK inhibitors in resistant cases
Topical agents: Topical steroids or calcineurin inhibitors for cutaneous lesions
Malignancy Surveillance
Age and gender-appropriate malignancy screening at baseline screening and annual review for 3–5 years
Interstitial Lung Disease
Immunosuppression and pulmonary monitoring
Supportive
- Dietitian (if dysphagia), physiotherapy, speech and language therapy
Dermatomyositis Cheat Sheet
| Domain | Summary |
|---|---|
| Genetics / Aetiology | Idiopathic inflammatory myopathy with autoimmune and paraneoplastic associations; triggered by infection, malignancy, or drugs. |
| Epidemiology | Incidence ~1 per 100,000; bimodal peaks (childhood & mid-adulthood); F > M. |
| Pathophysiology | Complement-mediated microangiopathy → muscle fibre necrosis and perifascicular atrophy; immune complex deposition in skin and muscle vessels. |
| History | Proximal muscle weakness, photosensitive rash (heliotrope, Gottron’s papules), dysphagia, dyspnoea, fatigue. |
| Examination | Symmetrical proximal weakness, heliotrope rash, Gottron’s papules, V-sign/Shawl sign, mechanic’s hands, nailfold erythema. |
| Differentials | Polymyositis, SLE, systemic sclerosis, drug-induced myopathy. |
| Investigations | CK ↑, myositis antibodies, EMG, MRI, muscle biopsy, age-appropriate malignancy screen, HRCT if ILD. |
| Management | Corticosteroids ± immunosuppressants, IVIG or biologics if refractory, physiotherapy, sun protection, cancer surveillance. |
| Complications | Interstitial lung disease, dysphagia, respiratory failure, cardiomyopathy, associated malignancy (ovarian, lung, GI). |



























































{kind=link}
{kind=link}