
Cardiovascular Station
Mechanical Valve Replacement
Important Physical Signs
General:
- Age (young – Connective Tissue Disease, congenital heart disease // old – degenerative valvular
disease)
Peripheral: (hands – arms – face – neck – torso)
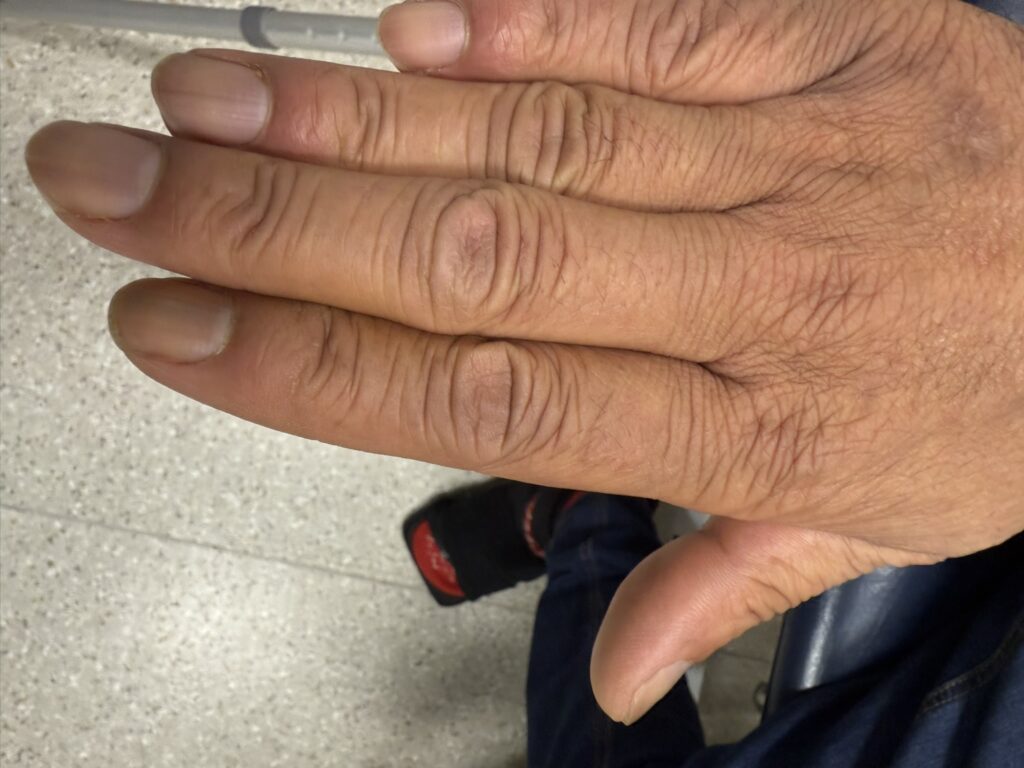
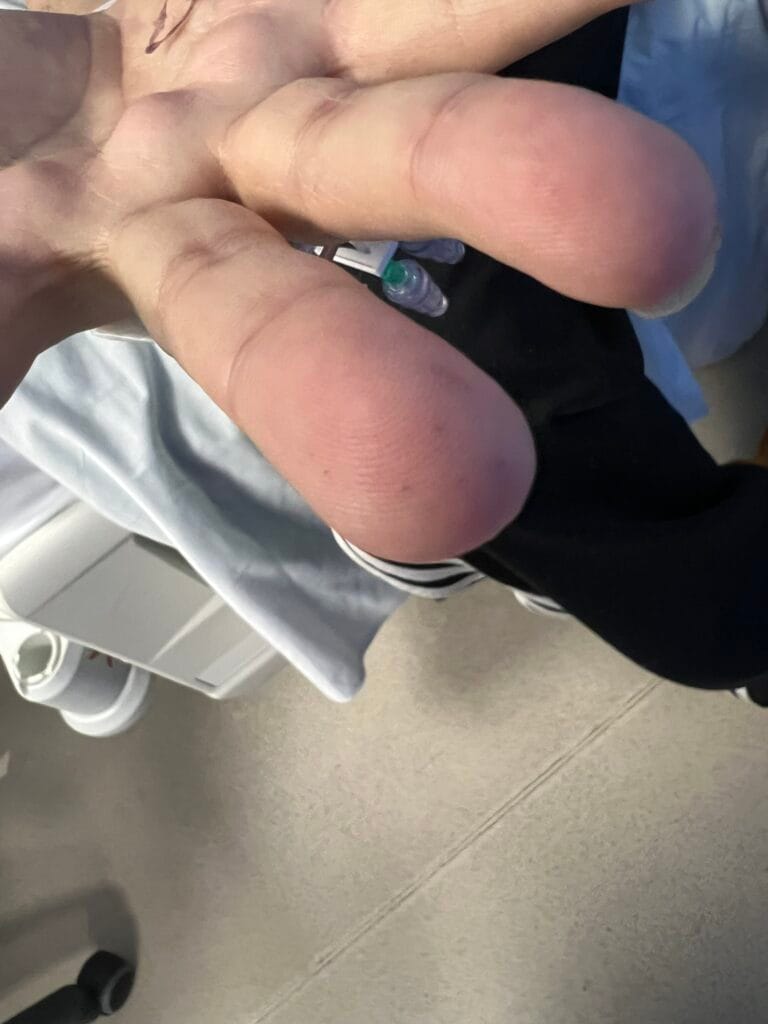
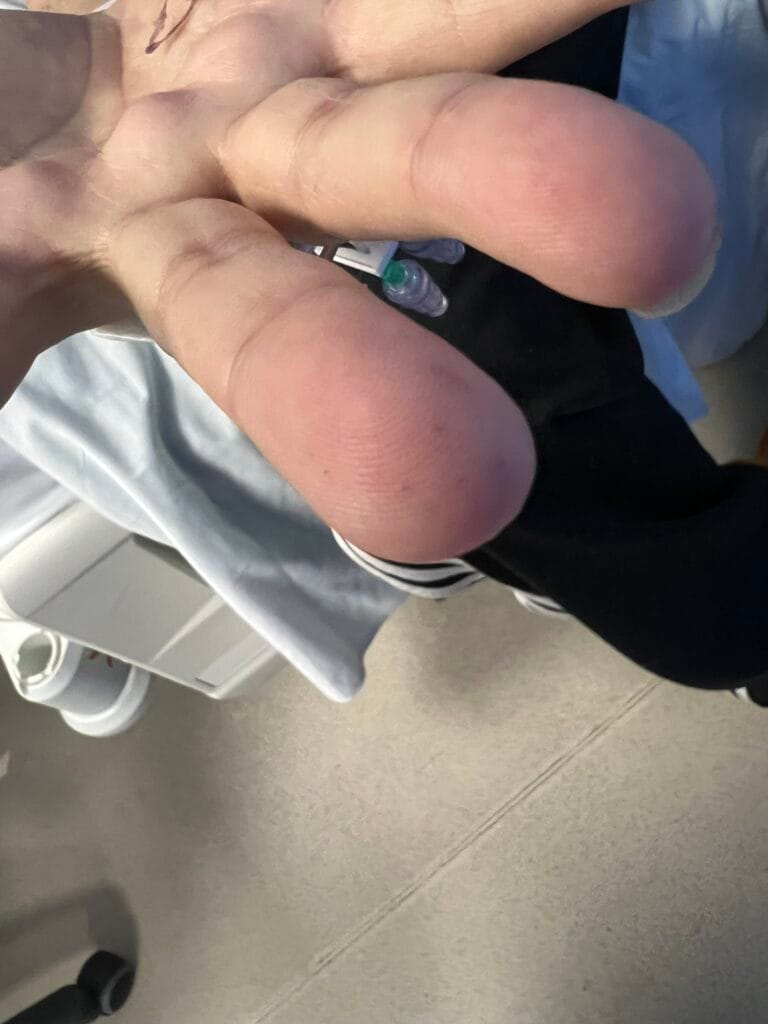
- Hands
- Peripheral cyanosis (blue finger pulp discolouration cyanotic heart disease)
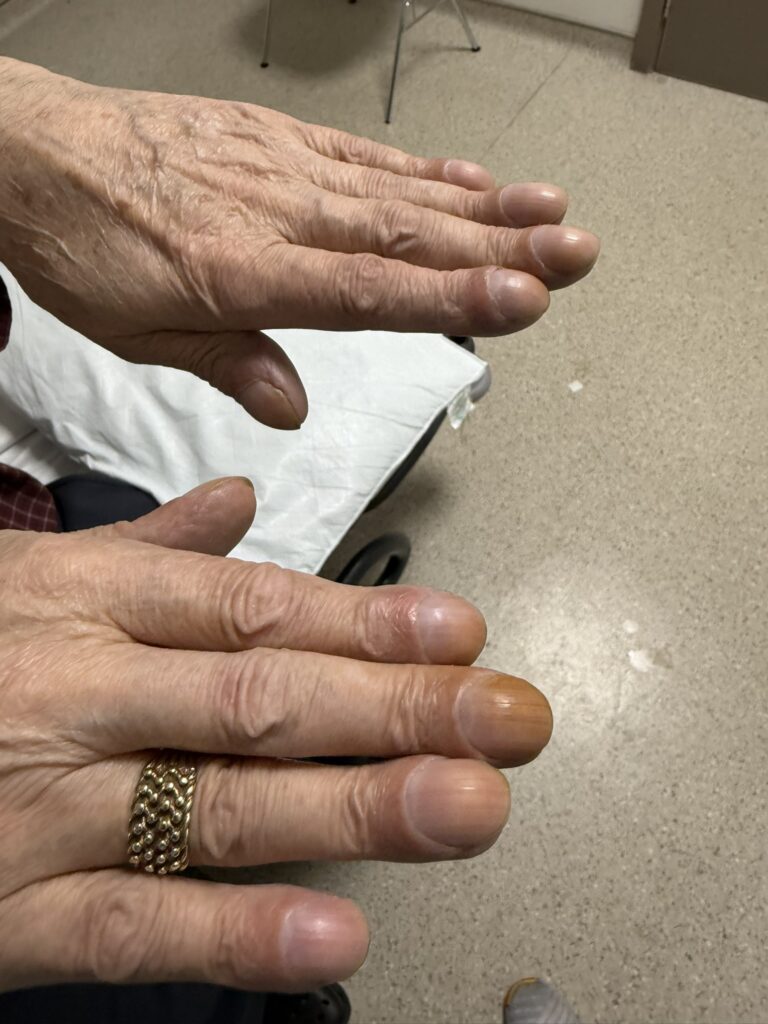
- Tar-stained fingers (check between index and middle fingers smokers)
- Clubbing (congenital heart disease)
- Radial pulse (rhythm – AVN pathology common in calcific degenerative disease)
- Peripheral stigmata of infective endocarditis (splinter haemorrhages, Janeway lesions, Osler Nodes)
- Arms
- Arm length span (increased in CTD – Marfan’s, ED, Pseudoxanthoma)
- Bruising (warfarin)
- Face
- General
- Mitral facies (mitral stenosis)
- Eyes
- Conjunctival pallor or jaundice (mechanical macroangiopathic haemolysis)
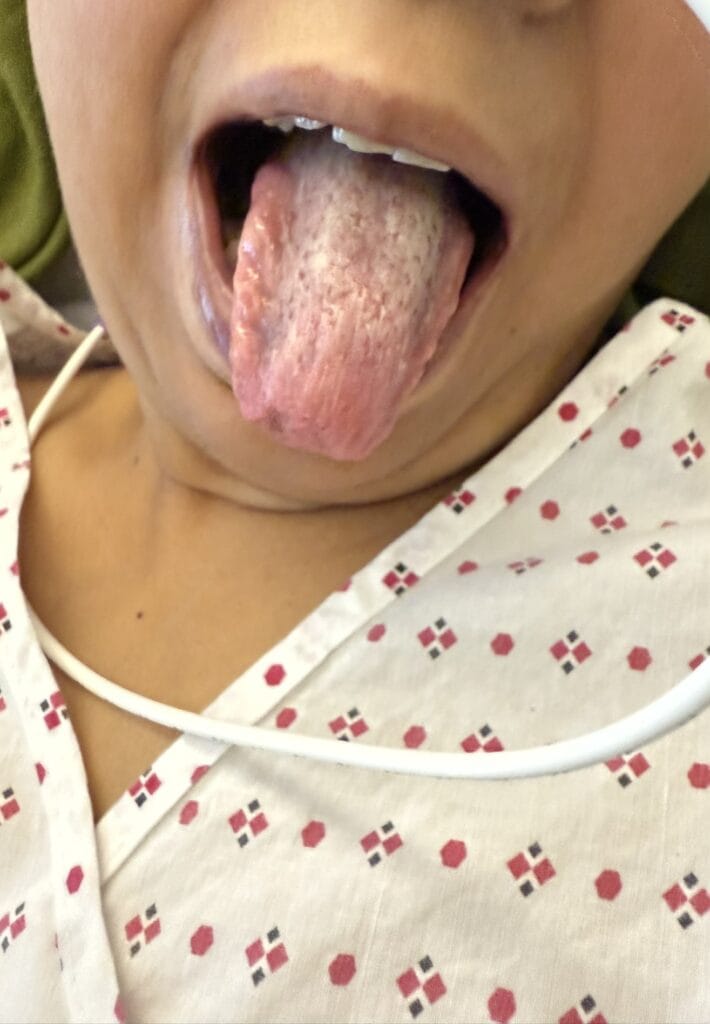
- Mouth
- Central cyanosis under tongue (congenital heart disease)
- High-arched palate (CTD)
- Neck
- JVP (right heart failure)
- Carotid pulse
- General
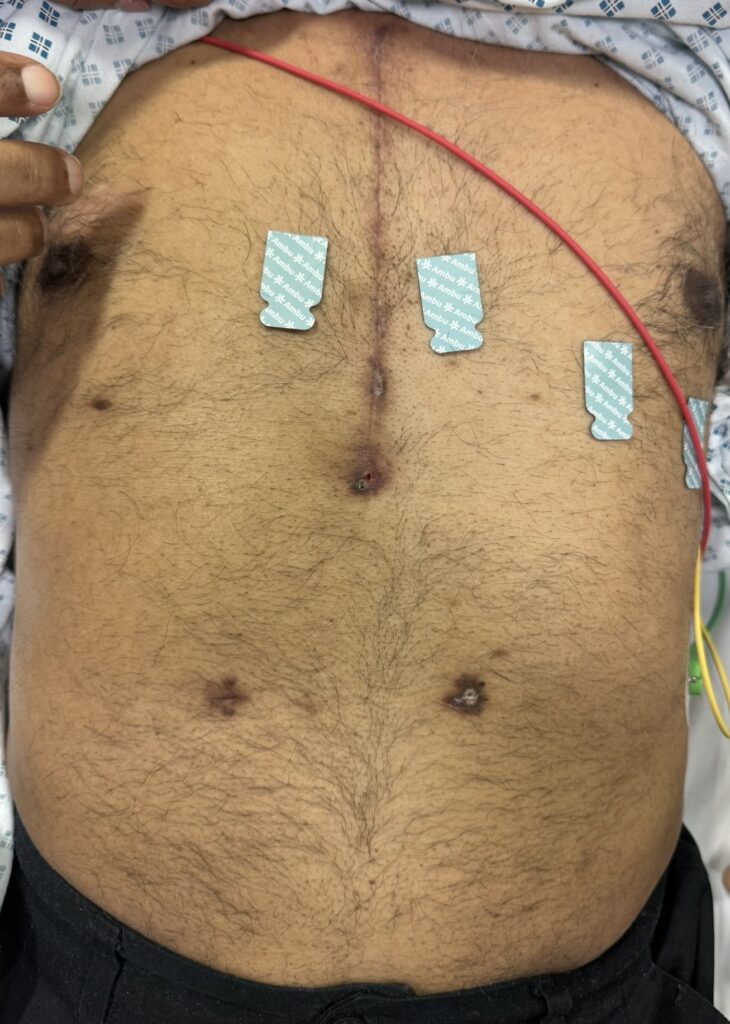
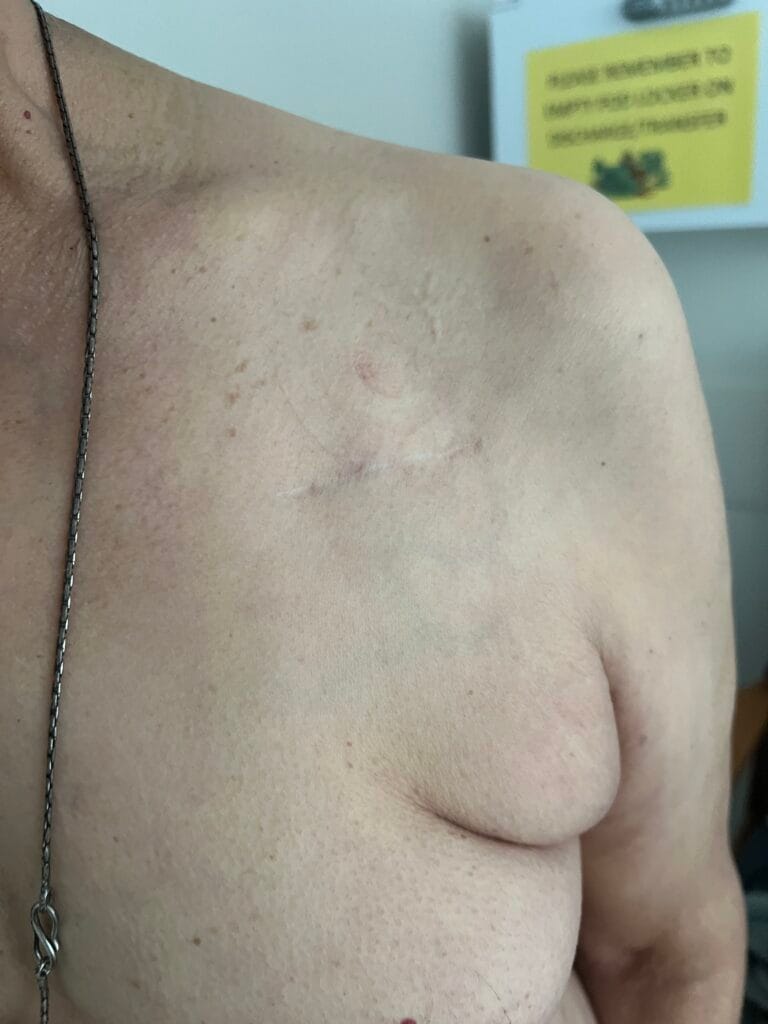
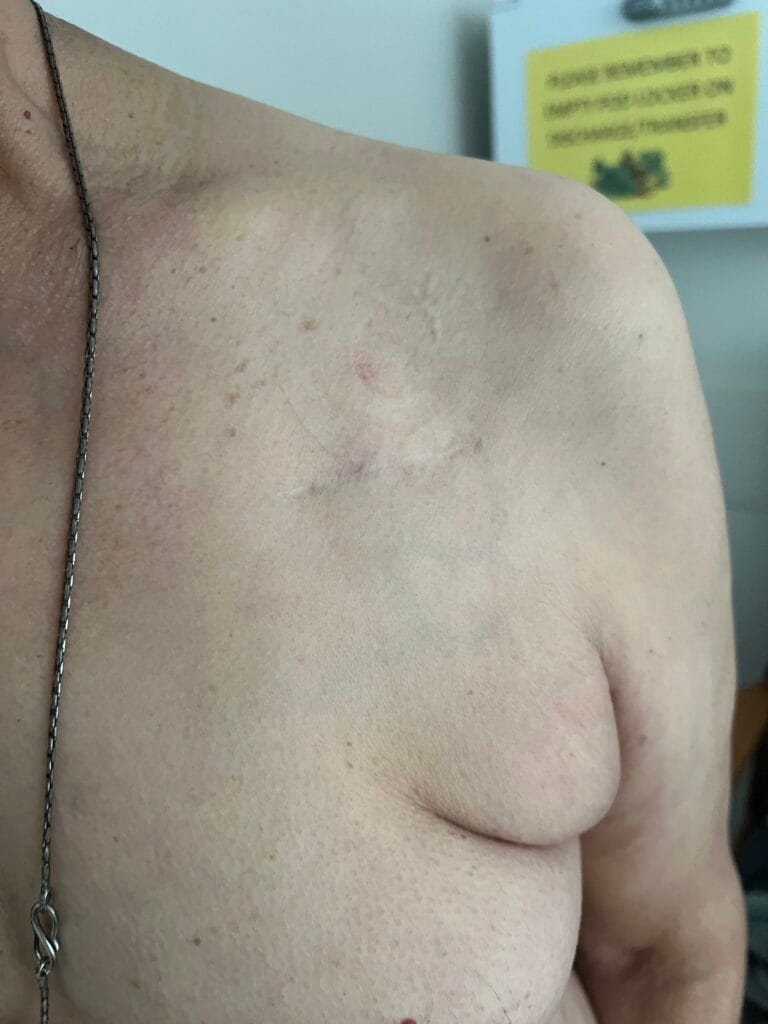
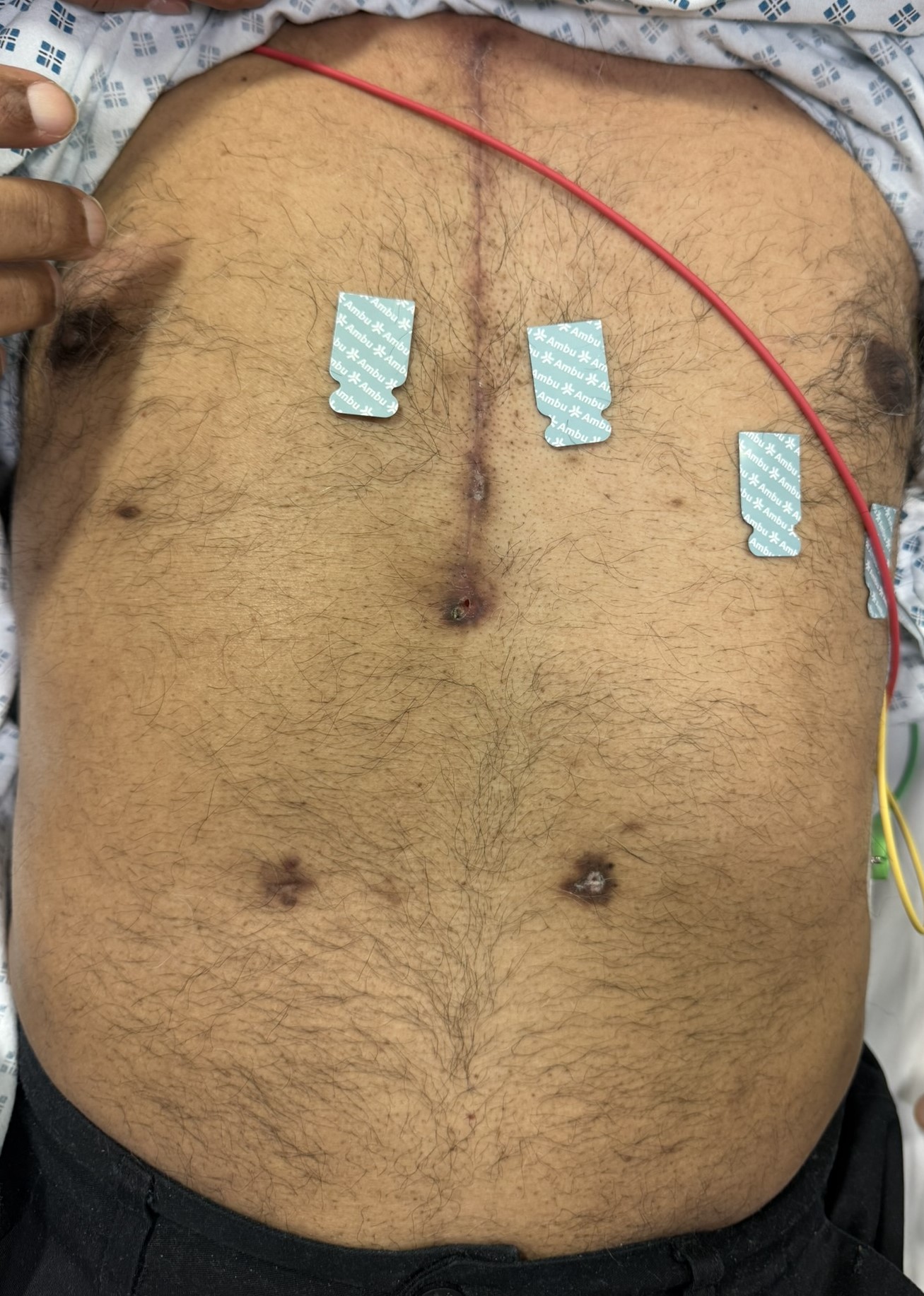
- Torso
- Palpable heaving apex (LVH)
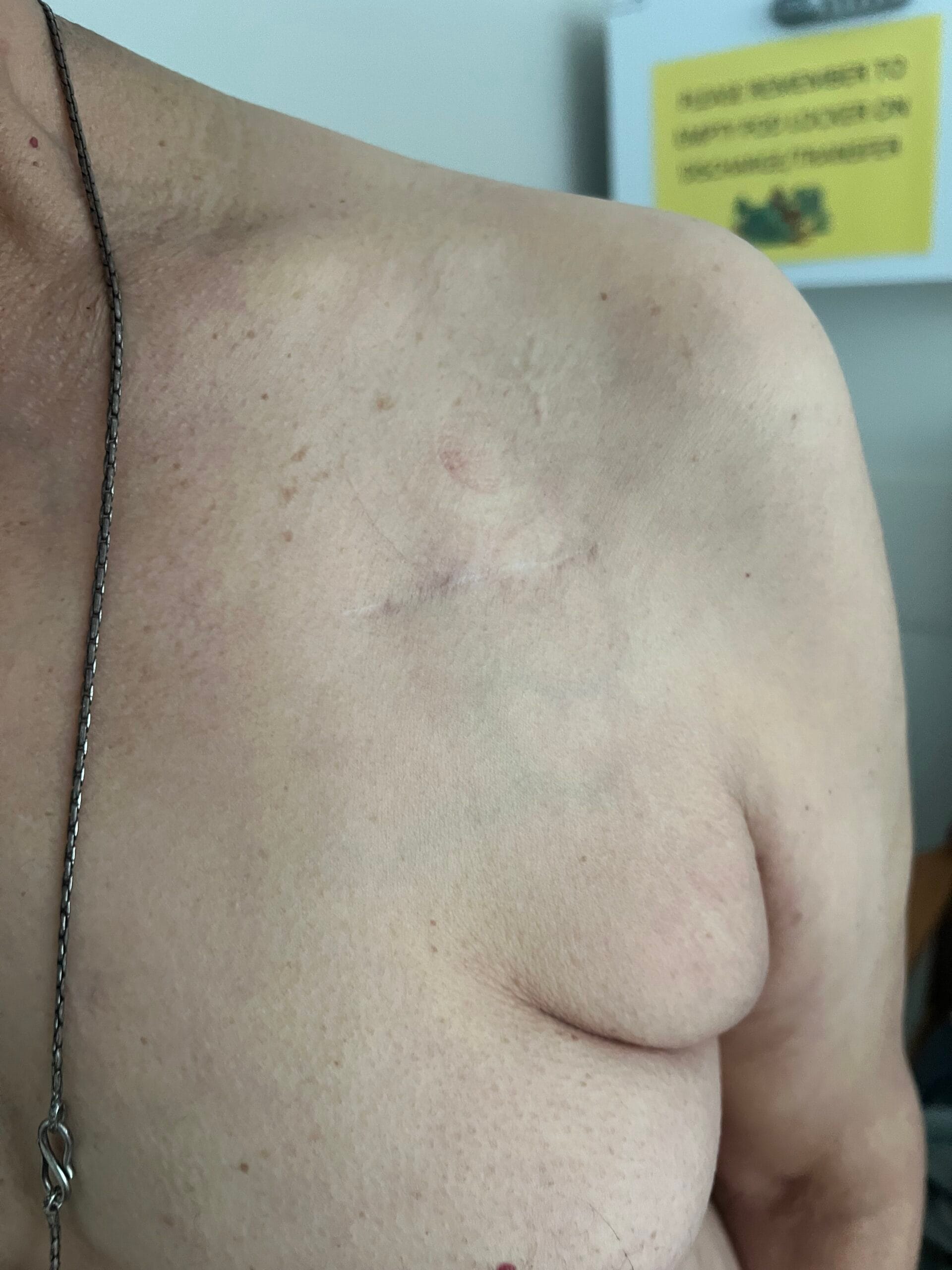
- Midline sternotomy scar (valve replacement +/- CABG)
- Infraclavicular scar (cardiac device insertion)
- Legs
- Vein harvesting scar (CABG)
- peripheral oedema🎬
Chest:
- Time heart sounds with carotid pulse
- Metallic Click with or right before pulse = Mechanical Mitral Valve Replacement🔊
- Loudest at mitral region
- Metallic click after pulse = Mechanical Aortic Valve Replacement🔊
- Loudest at aortic region
- Metallic click before and after pulse = Double Mechanical Valve Replacement🔊
- Aortic click loudest at aortic region and mitral click loudest at mitral region
- Metallic Click with or right before pulse = Mechanical Mitral Valve Replacement🔊
Presentation:
Diagnosis: Clinical findings are consistent with mechanical aortic valve replacement as evidenced by:
Most pertinent positive findings are: [Important Physical Signs]
Audible click with unaided ear
Loud aortic component of second heart sound with a prosthetic click
Loudest in the aortic region
Ejection systolic flow murmur (physiological)
Important negative findings include:
No evidence of peripheral stigmata of infective endocarditis
No signs of bruising secondary to over-anticoagulation
No evidence of acute cardiac decompensation (pulmonary oedema, peripheral oedema🎬)
No evidence of right heart failure with no overt JVP rise🎬, no RV heave and no peripheral oedema🎬
No evidence of mechanical microangiopathic haemolytic anaemia (conjunctival pallor, icterus)
Peripheral stigmata of infective endocarditis (splinter haemorrhages, Janeway lesions, Osler Nodes)
Overall this patient has had an aortic mechanical valve replacement which appears to be functioning well with
no evidence of prosthetic valve complications.
Differential Diagnosis:
Differential diagnosis include other causes of a loud second heart sound:
- Bioprosthetic valve replacement (no metallic click)
- Loud A2 secondary to systemic hypertension
- Loud P2 secondary to pulmonary hypertension
Clinical Judgement:
Bedside tests:
- ECG – looking for LVH, AV node disease (arrhythmias and heart block), paced rhythm post-surgery
Check pacemaker function (if pacemaker in-situ)
Blood investigations:
- FBC (anaemia in mechanical microangiopathic haemolytic anaemia)
- Inflammatory markers (raised in IE)
- Urea and electrolytes (baseline function)
Liver function tests (baseline function)
Imaging Studies:
- CXR – check for cardiomegaly, pulmonary oedema
- ECHO – left ventricular diameter, ejection fraction
Management
- MDT approach following referral to specialist cardiology centre
- Treat underlying cause
- Conservative (manage cardiovascular risk factors)
- Patient Education
- Lifestyle interventions – alcohol cessation, smoking cessation, encourage physical activity,
balanced diet
- Medical
- Anti-coagulation (No DOACs indicated)
- Warfarin
- Mitral Valve = INR 2.5 – 3.5
- Aortic valve = INR 2.0 – 3.0
- Warfarin
- Anti-coagulation (No DOACs indicated)
Surgical
Indications for Mechanical Valve Replacement:
- Aortic valve pathology (calcific aortic valve)
- Congenital aortic valve pathology (bicuspid aortic valve)
- Aortic root disease with aortic regurgitation (common in Marfan Syndrome)
- Rheumatic heart disease
Dilated cardiomyopathy with functional mitral regurgitation
Complications of mechanical valves:
- Valvular failure (evident as regurgitant murmur on auscultation)
- Acute endocarditis (peripheral stigmata, new murmur, fever, inflammatory markers)
- Mechanical Microangiopathic Haemolytic Anaemia
- Bleeding secondary to warfarin over-anticoagulation
Cerebrovascular events (embolic phenomena)
Difference of Mechanical vs Bioprosthetic Valves:
- Durability of mechanical valves (25 years vs 15 years) hence preferred in younger patients
- Lifelong warfarin anticoagulation with mechanical valve replacement
- Higher risk of bleeding with mechanical valve replacement
- Higher risk of thromboembolism with mechanical valve replacement
- Lower risk of subsequent valve repair or replacement with mechanical valve replacement



























































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}