Consultations
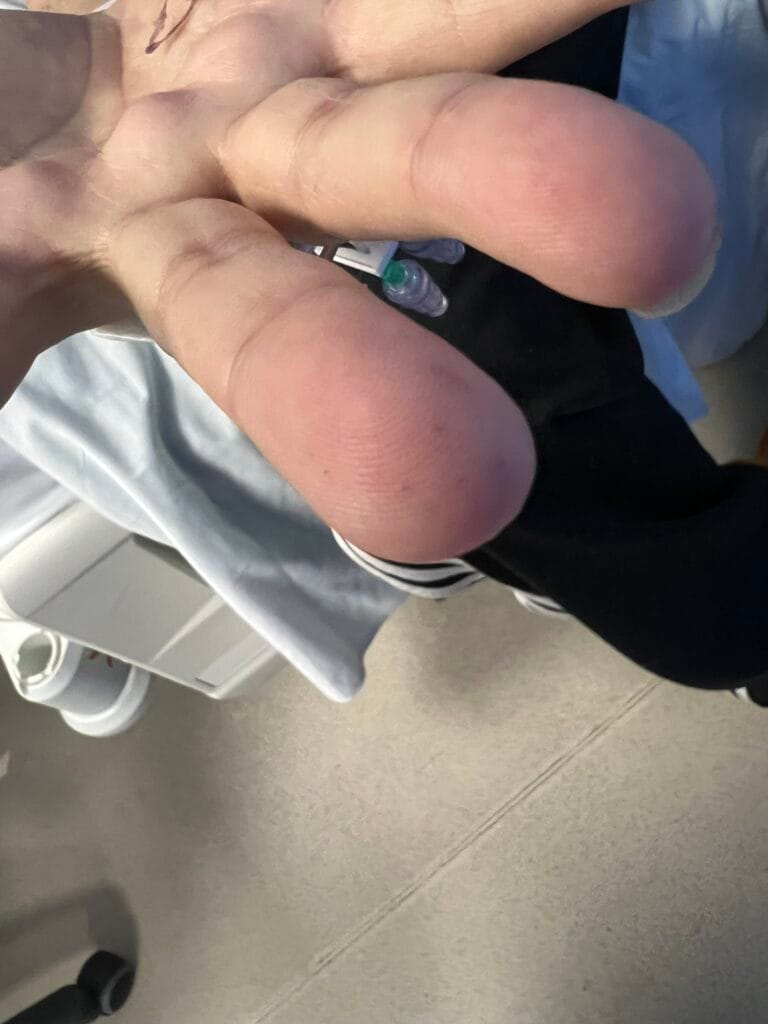
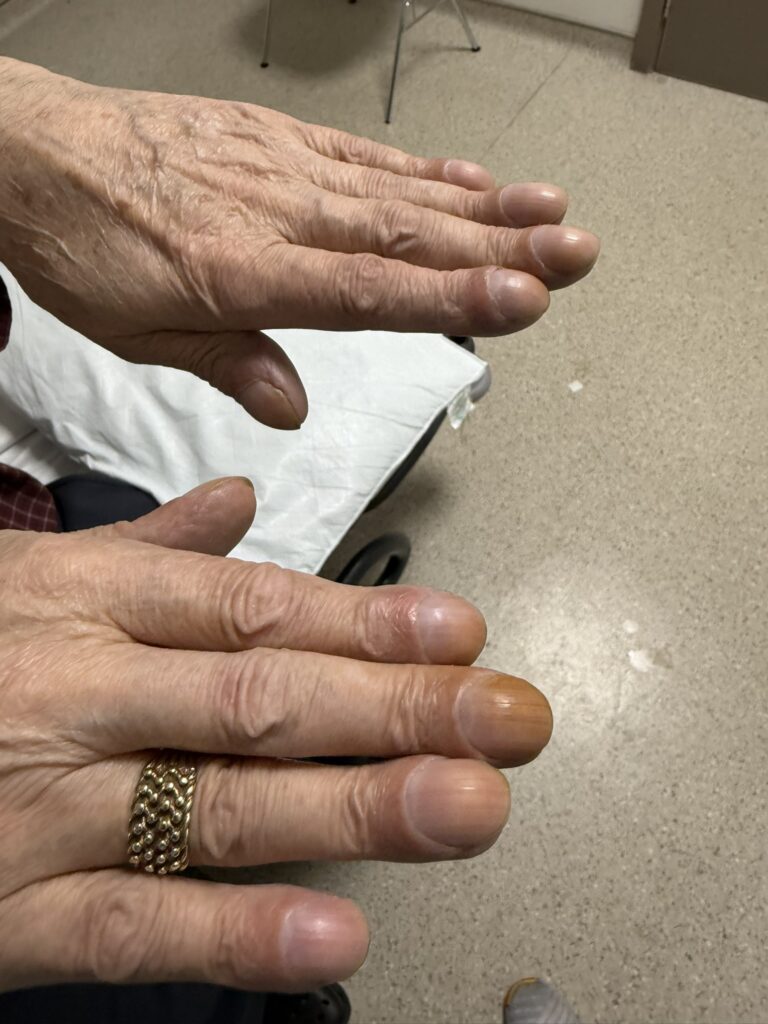
Ptosis
In Station 5 you may be asked to assess a patient presenting with eyelid drooping, double vision, or limb weakness.
Station Instructions: Please assess this patient who has noticed drooping of their eyelid and double vision.
1. Key History-Taking Points
Timing & Character
- Onset: since when, sudden vs gradual onset, intermittent vs constant
- Progression: getting worse over time?
- Diurnal variation: worse at the end of the day (classic for myasthenia gravis)
- Laterality: one or both eyelids affected
Ocular & Bulbar Symptoms
- Double vision: is it also worse at the end of the day? (fatiguable diplopia = myasthenia)
- Speech disturbance: slurring, nasal voice, voice fading with prolonged speech
- Difficulty swallowing: dysphagia, choking, nasal regurgitation
- Facial muscle weakness
Limb Weakness & Fatiguability
- Weakness of arms or legs — is it fatiguable (worse after exercise or as day progresses)?
- Shortness of breath: myasthenic crisis may impair respiratory muscles — a medical emergency
Myasthenia-Specific: Triggers & Precipitants
- Recent infection (commonest precipitant of myasthenic crisis)
- Drugs: recent antibiotics (aminoglycosides, fluoroquinolones), beta-blockers, calcium channel blockers, penicillamine (can induce MG)
- Low potassium (medication, poor intake)
Myotonic Dystrophy Screen
- Premature frontal balding
- Cataracts (visual disturbance)
- Heart problems (palpitations, syncope — cardiomyopathy, arrhythmia, heart block)
- Lung problems, recurrent chest infections (aspiration, bronchiectasis)
- GI problems: dysphagia, constipation, diarrhoea, reflux
- Diabetes (polyuria, polydipsia)
- Excessive daytime sleepiness (hypersomnia)
- Family history of weakness — anticipation means it may be worse in children
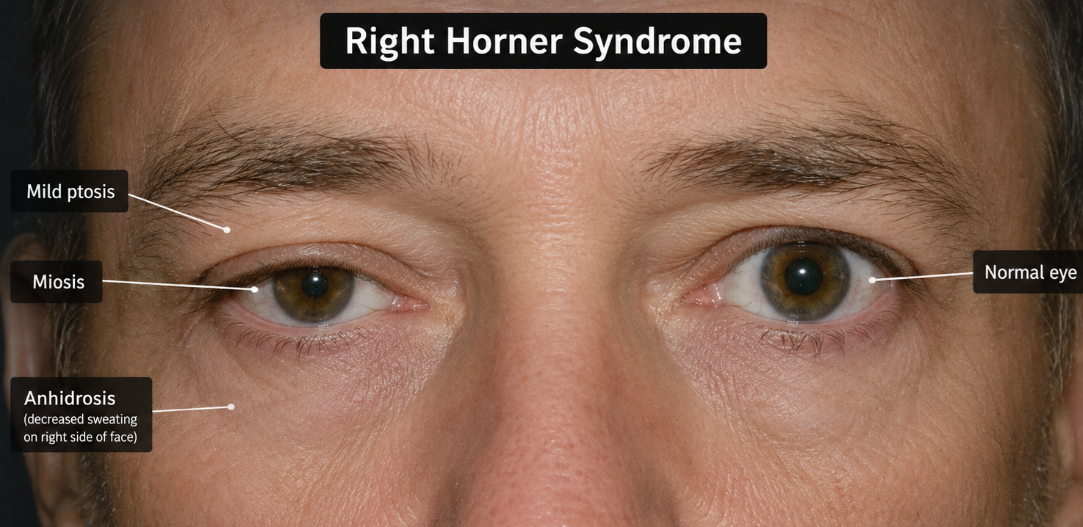
Horner’s Syndrome Screen
- Pancoast tumour: cough, haemoptysis, chest pain, significant smoking history, weight loss, night sweats
- Anhidrosis: loss of sweating on face, arms or trunk (localises the lesion)
- Neck: any trauma or surgery to the neck, neck pain
- Headache: carotid dissection (sudden severe neck or head pain), cavernous sinus pathology
General Neurological Screen
- Sensory loss, headache, seizures, tremor, unsteadiness
- Vascular risk factors (stroke causing CN III palsy or Horner’s): hypertension, diabetes, hypercholesterolaemia, smoking, atrial fibrillation
Past Medical, Drug & Family History
- PMH: autoimmune conditions (thyroid disease, RA, SLE, diabetes), cardiovascular risk factors
- Medications: include penicillamine specifically
- Family history: autoimmune disease, muscle weakness, myotonic dystrophy
2. Key Examination Findings
Inspection
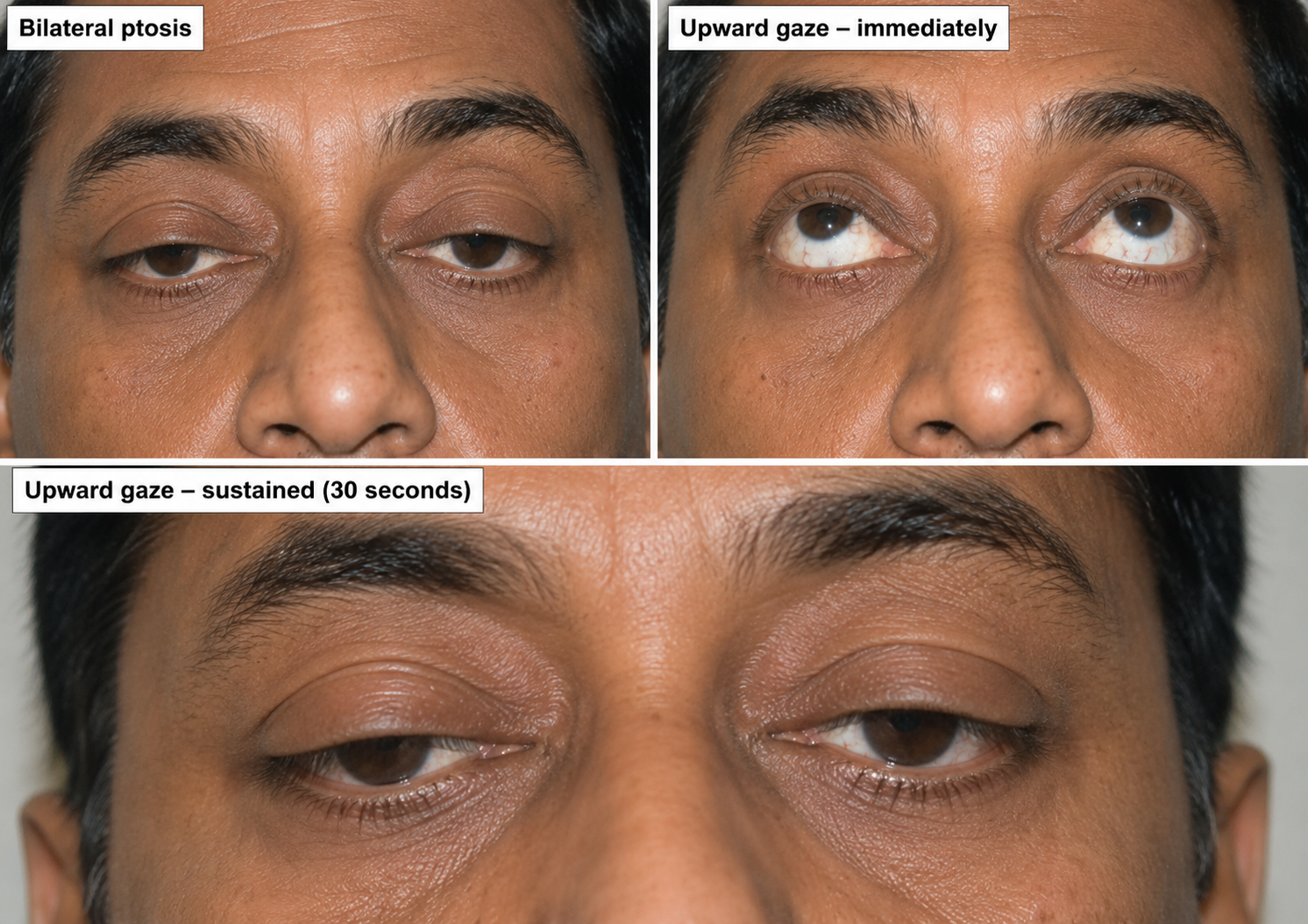
- Ptosis: unilateral vs bilateral, symmetrical vs asymmetrical, partial vs complete
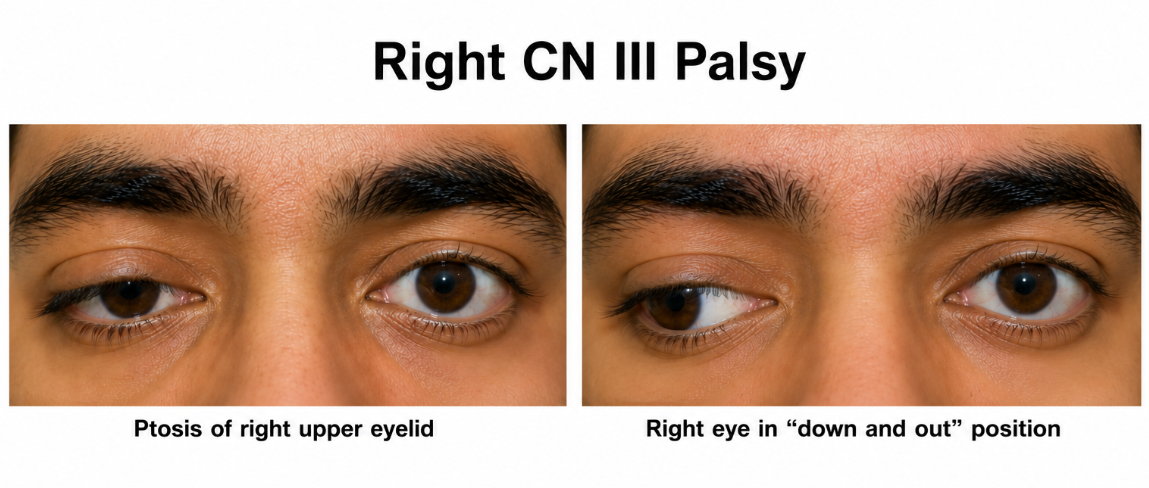
- Eye position: abducted and depressed = CN III palsy (unopposed lateral rectus and superior oblique)
- Pupils:
- Dilated, unreactive = CN III palsy (loss of parasympathetic supply) — compressive cause until proven otherwise
- Small (miosis) with intact reflexes = Horner’s syndrome
- Normal size = myasthenia gravis, myotonic dystrophy
Eye Movements & Fatiguability
- Test all directions; ask patient if diplopia occurs
- Specifically test CN IV: ask to look down and inwards (superior oblique)
- Specifically test CN VI: ask to look laterally (lateral rectus)
- Observe for complex ophthalmoplegia
- Fatiguability test: ask patient to sustain upward gaze for 20 seconds — ptosis worsening = myasthenia gravis
- Ice pack test: apply ice to closed eyelid for 2 minutes — improvement in ptosis suggests myasthenia gravis
Pupils & Visual Examination
- Pupil reflexes (direct and consensual)
- RAPD (relative afferent pupillary defect — Marcus Gunn test)
- Visual fields
- Visual acuity
- Fundoscopy
- Temporal artery palpation if age >50 (giant cell arteritis — a cause of CN III palsy and visual loss)
Other Cranial Nerves
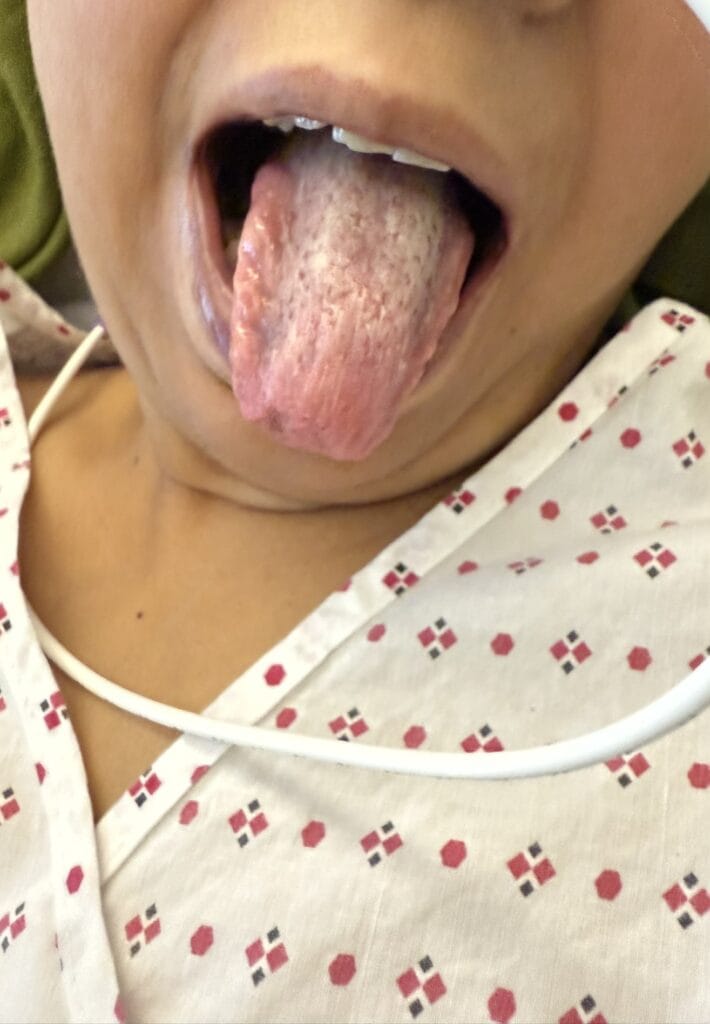
- CN V (facial sensation), CN VII (facial movements), CN VIII (hearing), CN IX/X (palate movement, gag), CN XI (trapezius/SCM), CN XII (tongue)
Myasthenia-Specific Tests
- Eye closure (peek sign): ask to close eyes — inability to sustain tight closure, lids slowly part
- Lip closure
- Neck flexion and extension against resistance
- Jaw supporting sign: patient supports their jaw with hand to aid mouth closure
- Fatiguable proximal limb weakness: test elbow flexion/extension, shoulder abduction; ask to perform 10–20 repetitions (“chicken wing” arm exercises) then retest — weaker after exercise
- Speech fatiguability: ask to count to 50 — voice fades or becomes nasal
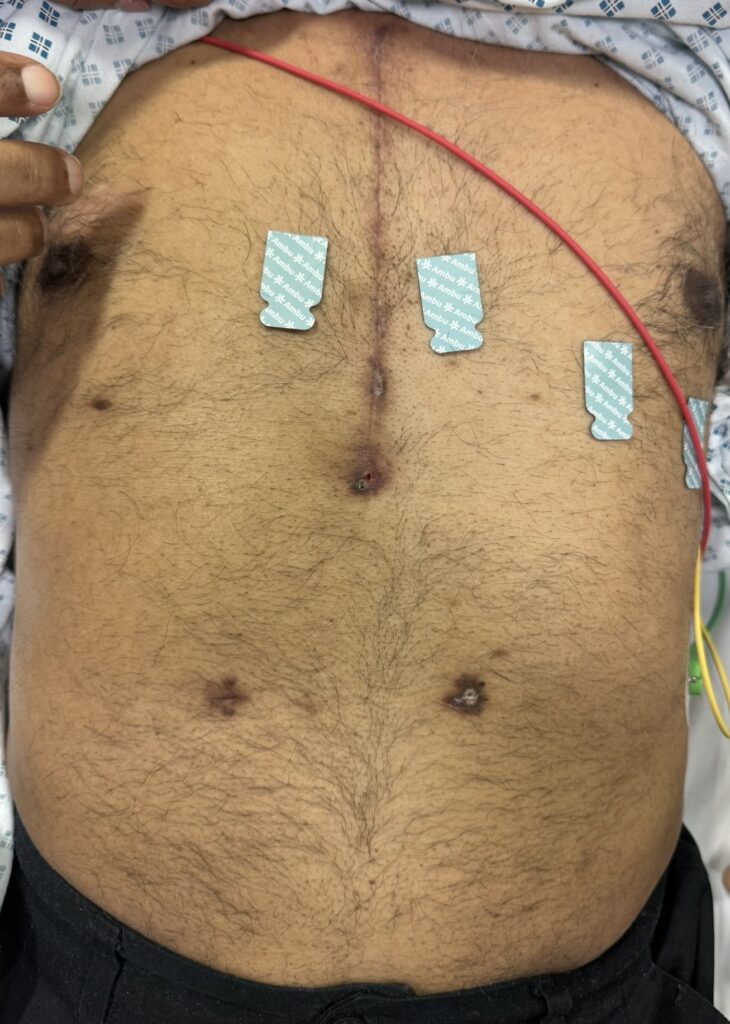
- Inspect for: midline sternotomy scar (thymectomy), Cushingoid appearance (steroid use), NG tube or gastrostomy (PEG), spirometer at bedside
- Respiratory: assess chest expansion; offer FVC measurement
- Look for associated autoimmune conditions: thyroid signs, RA hands, SLE rash, diabetic fingerprick marks
Myotonic Dystrophy-Specific Tests
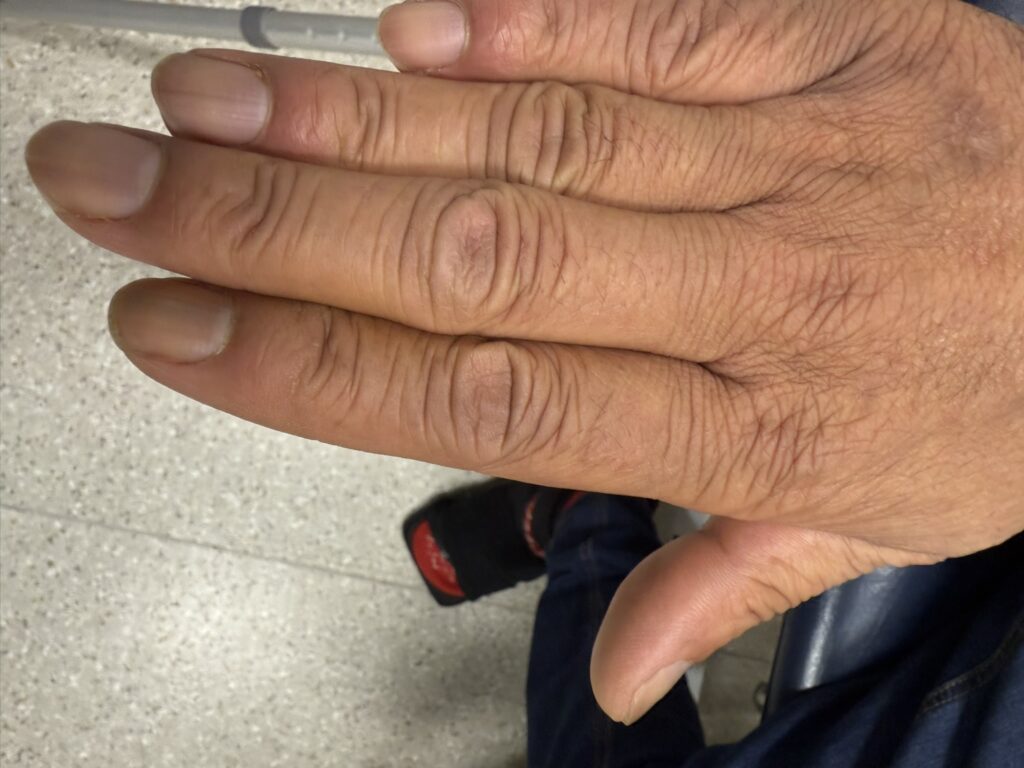
- Grip myotonia: shake patient’s hand — delay before grip release; ask to rapidly open and close fist
- Percussion myotonia: tap thenar eminence with tendon hammer — thumb flexes and sustains
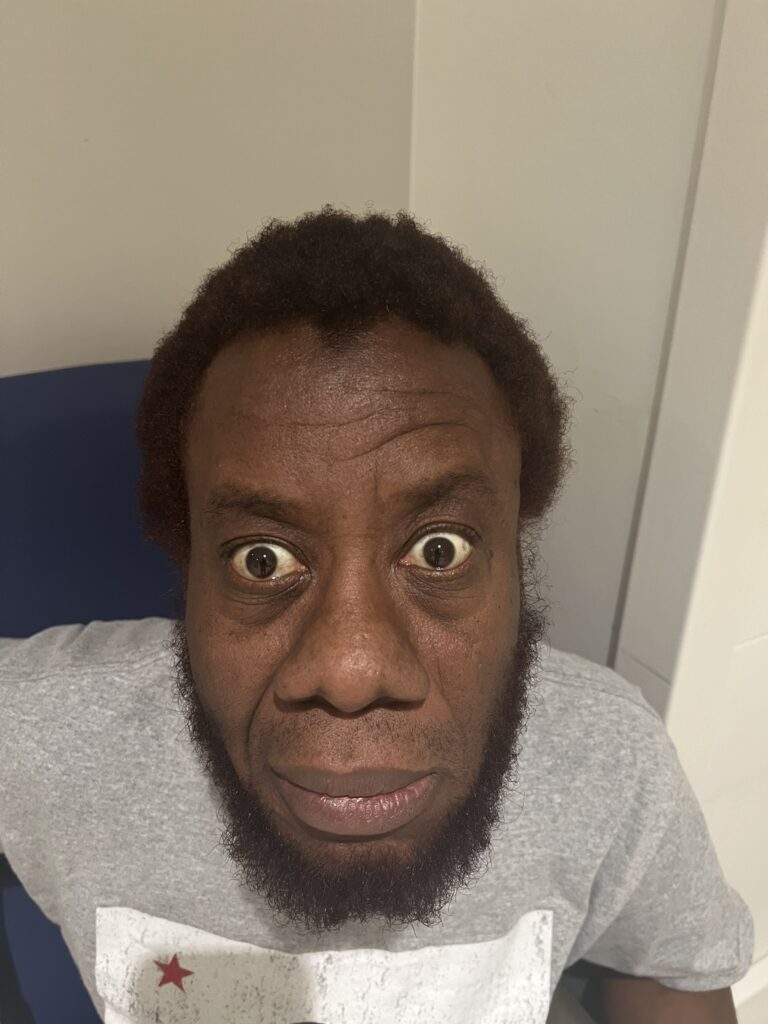
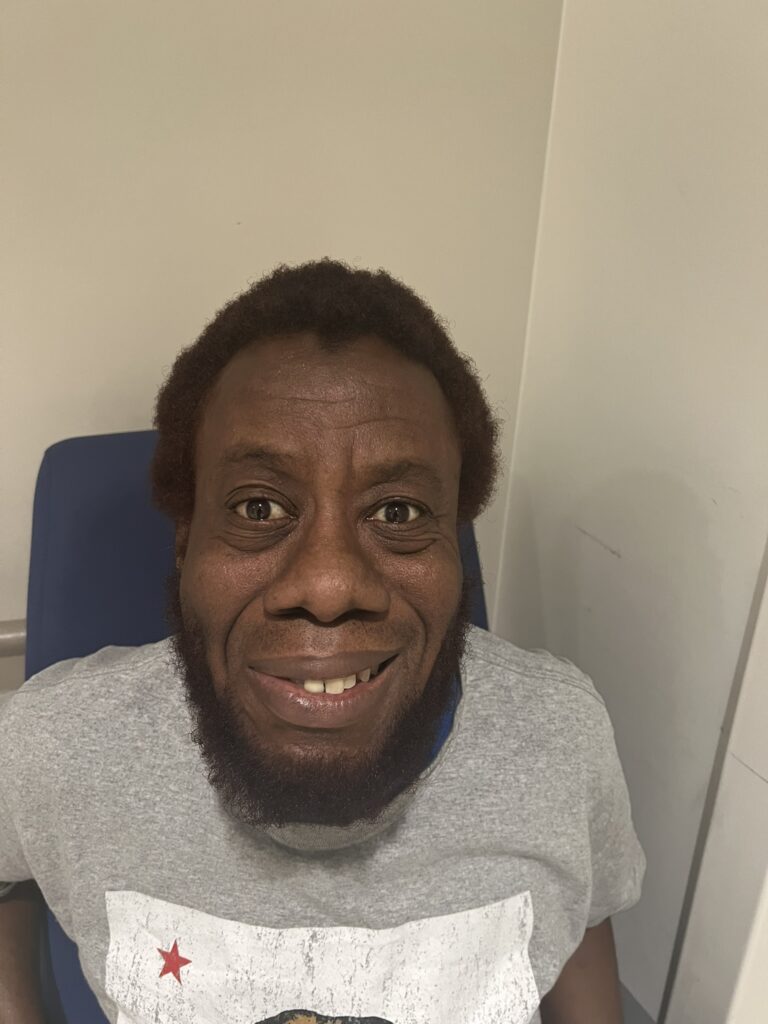
- Face and neck: frontal balding, myopathic facies (long, wasted face), bilateral ptosis, cataracts; palpate temporalis and masseter on clenching (wasted and weak); palpate sternocleidomastoids (wasted and weak — swan neck); goitre
- Delayed eye opening: ask to close eyes tightly then open — delayed
- Chest: gynaecomastia, apex beat, pacemaker scar, auscultate heart (murmur), auscultate lungs (bronchiectasis)
- Pulse and diabetic fingerprick marks
Horner’s Syndrome-Specific Examination
- Hands: wasting of small muscles (T1), APB power, FDI power, sensation C8–T1, clubbing, DM fingerprick marks (Pancoast)
- Neck: scars (thyroidectomy/neck surgery), carotid pulse, lymphadenopathy, goitre, tracheal deviation, carotid bruits
- Axilla: scars (apical surgery)
- Chest: auscultate lungs (apical signs of Pancoast), heart sounds
General Neurological Assessment
- Tone, power, sensation (note: sensation is normal in myasthenia and myotonic dystrophy), reflexes (reduced/absent in myotonic dystrophy), coordination
Viva presentation template (myasthenia gravis): “I think this patient has myasthenia gravis as evidenced by muscle weakness with fatiguability. There is bilateral asymmetrical fatiguable partial ptosis. There is diplopia and complex ophthalmoplegia. There is bilateral facial muscle weakness with weak eye closure, lip seal and a positive peek sign. There is weakness of neck extension and a positive jaw supporting sign. There is proximal limb weakness which is fatiguable. There is dysarthria and dysphonia. I observed a midline sternotomy scar and signs of steroid toxicity. Chest wall expansion was reduced. I looked for evidence of other autoimmune disorders.”
ICE explanation template (myasthenia gravis): “There are many causes of eyelid drooping and double vision. I think you may have a condition called myasthenia gravis, in which the muscles become weak and tired. The eye muscles are commonly affected, causing double vision and drooping that is often worse at the end of the day. It is caused by a problem with the immune system. It can also affect the face, neck, swallowing, speech and breathing, and sometimes causes weakness in the arms and legs. Infections or certain medications can trigger the symptoms to worsen. I will arrange blood tests, nerve and muscle tests, and breathing tests, and I will refer you to a neurologist. If it is myasthenia gravis, effective treatments are available.”
3. Specific Investigations
Bloods
- AChR antibodies: positive in 80–90% of generalised MG
- Anti-MuSK antibodies: positive in 10–20%, often positive when AChR negative
- Antistriatal muscle antibodies: positive in ~90% with thymoma
- TFTs: Graves’ disease in 5% of MG; exclude thyroid eye disease as cause of ophthalmoplegia
- FBC, CRP: screen for infection (myasthenic crisis trigger)
- CK: normal in MG; elevated in myopathies
- U&E: hypokalaemia worsens MG
- Glucose / HbA1c: diabetes (mononeuritis multiplex, myotonic dystrophy)
Diagnostic Tests for Myasthenia
- Tensilon (edrophonium) test: IV anticholinesterase — look for improvement in ptosis within 30 seconds, lasting 2–3 minutes; requires cardiac monitoring (bradycardia, heart block, asystole) and resuscitation equipment
- Ice pack test: ice applied to closed eyelid for 2 minutes — ptosis improves in MG (cooling improves neuromuscular transmission)
Neurophysiology
- Repetitive nerve stimulation: decremental response in amplitude with repeated stimulation (MG); incremental response (LEMS)
- Single-fibre EMG: increased jitter — most sensitive test for MG
- EMG (myotonic dystrophy): dive-bomber pattern — waxing and waning potentials; repetitive discharges with minor stimulation
Imaging & Respiratory Function
- CT/MRI thymus: essential in all MG — 10–15% have thymoma (10% malignant), 90% have thymic hyperplasia
- CXR: mediastinal mass (thymoma), Pancoast tumour (apical lung mass), cardiomegaly (myotonic dystrophy)
- Spirometry (FVC): monitor respiratory muscle involvement; FVC <1 L = critical
- Saturations, ABG
- For Horner’s: MRI brain and spine (central), CT thorax (preganglionic — Pancoast), MRI/A head and neck + Carotid Doppler (postganglionic — dissection, cavernous sinus)
- For CN III palsy: urgent MRI/MRA/CTA if pupil dilated, brainstem signs, other CNs involved, or acute severe headache (posterior communicating artery aneurysm)
Pharmacological Pupil Tests (Horner’s Syndrome)
- Cocaine 4%: normal pupil dilates; affected pupil does not dilate at 60 minutes (confirms Horner’s)
- Apraclonidine 0.5%: normal pupil constricts; affected pupil dilates relatively (denervation hypersensitivity — confirms Horner’s)
- Hydroxyamphetamine 1%: pupil dilates if central or preganglionic lesion; does not dilate if postganglionic lesion (localises lesion)
4. Management
Myasthenia Gravis
- Identify and treat precipitant: infection, culprit drugs, medication non-compliance, hypokalaemia
- SALT assessment and NG/PEG feeding if bulbar involvement
- Anticholinesterases: pyridostigmine (first-line symptomatic therapy)
- Immunosuppression: prednisolone (with gastro- and bone protection); steroid-sparing agents — azathioprine, mycophenolate mofetil
- Acute/crisis treatment: plasma exchange (plasmapheresis), IV immunoglobulin (IVIG)
- Thymectomy: recommended in thymoma and in generalised MG in patients under 65
- Neurology referral; monitor FVC regularly
Myotonic Dystrophy
- MDT: neurology, ophthalmology, cardiology, respiratory, gastroenterology, endocrinology, SALT, physiotherapy, OT, psychiatry, geneticist, GP
- Myotonia: phenytoin, quinine, procainamide, mexiletine
- Manage complications: pacemaker for heart block; treat diabetes and obstructive sleep apnoea
- Screen relatives (autosomal dominant; anticipation)
- Surgical: cataract removal; note anaesthesia is high risk in myotonic dystrophy
CN III Palsy
- If compressive (dilated pupil), brainstem signs, or acute severe headache: urgent MRI/MRA/CTA; neurosurgery referral for aneurysm coiling/clipping
- If pupil-sparing isolated CN III with vascular risk factors: optimise cardiovascular risk factors; no driving, climbing or heavy machinery; eye patch or prism for diplopia; review at 3 months; MRI if not recovered
Horner’s Syndrome
- Treat the underlying cause (localise lesion first — central/preganglionic/postganglionic)
- Urgent imaging if carotid dissection or Pancoast tumour suspected
Ptosis Cheat Sheet
| Domain | Summary |
|---|---|
| Differentials of Ptosis | Myasthenia gravis (bilateral), myotonic dystrophy (bilateral), Horner’s syndrome (unilateral, partial), CN III palsy (unilateral, complete or partial), oculopharyngeal muscular dystrophy (bilateral), mitochondrial disease e.g. Kearns-Sayre (bilateral) |
| Differentials of Complex Ophthalmoplegia | Myasthenia gravis, thyroid eye disease, oculopharyngeal muscular dystrophy, mononeuritis multiplex (diabetes), mitochondrial disease (Kearns-Sayre), Miller Fisher variant of GBS, cavernous sinus pathology, Wernicke’s encephalopathy, progressive supranuclear palsy |
| Myasthenia Gravis | Acquired autoimmune; anti-AChR antibodies (80–90%) at postsynaptic NMJ; thymus involved in 75% (10–15% thymoma, 90% thymic hyperplasia); 50% of thymoma patients develop MG; prevalence 1:10,000; females 20–35 yrs (autoimmune) or males >50 yrs (oculobulbar/thymoma); fatiguable weakness of extraocular, bulbar, facial, neck, limb muscles; 15% pure ocular; 20% pure bulbar; penicillamine can induce MG |
| MG Differentials |
• LEMS: presynaptic anti-VGCC antibodies; associated with malignancy (SCLC); no ophthalmoplegia or bulbar/respiratory involvement; proximal weakness improves with exercise; reduced reflexes that increase after exercise; autonomic and sensory features • Botulism: descending paralysis, dilated fixed pupils, no fever • Mitochondrial disease (Kearns-Sayre): ptosis, ophthalmoplegia, pigmentary retinopathy, heart block • Miller Fisher GBS: ataxia, areflexia, ophthalmoplegia; anti-GQ1b antibodies |
| Myotonic Dystrophy | Most common adult muscular dystrophy; CTG trinucleotide repeat expansion on chromosome 19; DMPK gene; autosomal dominant; shows anticipation; features: frontal balding, cataracts, bilateral ptosis, myopathic facies, temporalis/masseter wasting, swan-neck (SCM wasting), grip myotonia, cardiomyopathy/arrhythmia, diabetes, hypersomnia, GI dysmotility, bronchiectasis; EMG: dive-bomber pattern |
| CN III Palsy | Complete ptosis (compressive) or partial (medical/vascular); dilated unreactive pupil (compressive); eye abducted and depressed (unopposed LR/SO); diplopia all directions. Compressive causes: PCA aneurysm, uncal herniation, cavernous sinus. Medical (pupil-sparing): diabetes, hypertension, vasculitis, GCA, migraine. Urgent imaging if dilated pupil, sudden headache, or brainstem signs |
| Horner’s Syndrome | Partial ptosis, miosis (intact reflex), enophthalmos, anhidrosis. Central (loss of sweating face/arm/trunk): stroke, SOL, demyelination, syringomyelia → MRI brain/spine. Preganglionic (loss of sweating face): Pancoast, thyroidectomy, cervical rib → CXR/CT thorax. Postganglionic (no sweating loss): carotid dissection/aneurysm, cavernous sinus, cluster headache → MRI/A head+neck, carotid Doppler. Confirm with apraclonidine; localise with hydroxyamphetamine |
| Key Investigations | AChR Ab, anti-MuSK Ab, antistriatal Ab; TFTs; FBC, CRP, CK, U&E; tensilon/ice pack test; single-fibre EMG (most sensitive); CT/MRI thymus; FVC (respiratory monitoring); imaging tailored to suspected cause (MRI brain, CT thorax, MRI neck/carotid Doppler) |
| Management (MG) | Treat precipitant; pyridostigmine; prednisolone + steroid-sparing (azathioprine, mycophenolate); plasma exchange/IVIG for crisis; thymectomy; monitor FVC; neurology referral |
☐