Consultations
Marfan’s Syndrome
In Station 5 you may be asked to assess a patient presenting with chest pain, breathlessness, or visual disturbance.
Station Instructions: Please assess this tall patient who has presented with chest pain and breathlessness.
1. Key History-Taking Points
Cardiovascular Symptoms
- Chest pain: onset, character, radiation — tearing/ripping pain radiating to the back raises concern for aortic dissection
- Breathlessness: onset, exertional vs rest, orthopnoea, PND (aortic regurgitation, heart failure, mitral valve prolapse)
- Palpitations: arrhythmia (MVP, aortic regurgitation)
- Syncope or pre-syncope
- Known heart murmur or previous cardiac investigations
Respiratory Symptoms
- Sudden-onset pleuritic chest pain and breathlessness: spontaneous pneumothorax (tall, thin young patients at high risk)
- Cough, wheeze
Ocular Symptoms
- Visual disturbance, blurred or reduced vision (ectopia lentis, myopia)
- Monocular visual disturbance or loss (lens dislocation)
- Known short-sightedness (myopia is common in Marfan’s)
- Glasses or contact lens use
Musculoskeletal & Physical Features
- Tall stature, long limbs — has anyone commented on height?
- Joint hypermobility, joint pain, recurrent dislocations
- Back pain, spinal curvature (scoliosis, kyphosis)
- Flat feet (pes planus)
- Skin stretch marks (striae)
Neurological Screen
- Weakness or sensory disturbance in the limbs
- Bowel or bladder disturbance (dural ectasia — enlargement of the dural sac in the lumbosacral region)
- Headache, visual field disturbance
Past Medical, Drug & Family History
- PMH: previous aortic surgery, pneumothorax, lens surgery, cardiac investigations
- Medications: beta-blockers or ARBs (aortic surveillance treatment), anticoagulants
- Family history: Marfan’s syndrome is autosomal dominant — first-degree relatives affected? Any sudden cardiac death in the family (aortic dissection)?
- Exercise: current level — high-intensity exercise and contact sports should be avoided
2. Key Examination Findings
Standing
- Height: tall stature
- Arm span to height ratio: increased arm span (>1.05 arm span:height ratio)
- Kyphoscoliosis: inspect spine from behind and side
- Pes planus: inspect medial arches of both feet (flat feet)
Hands & Arms — Sitting
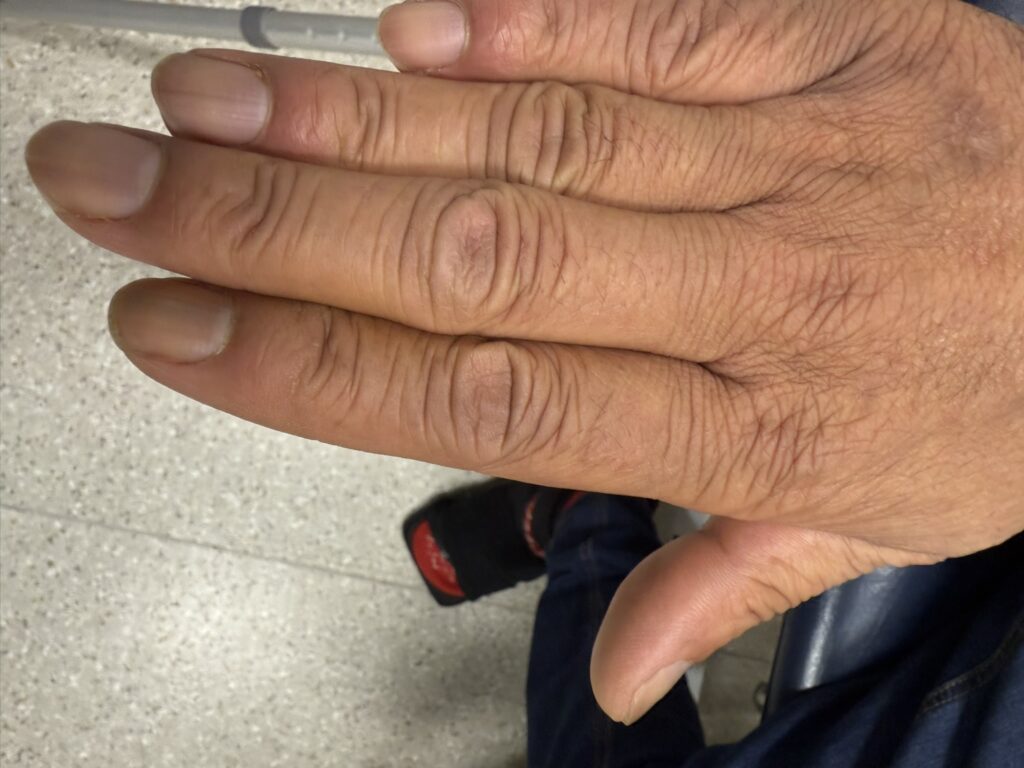
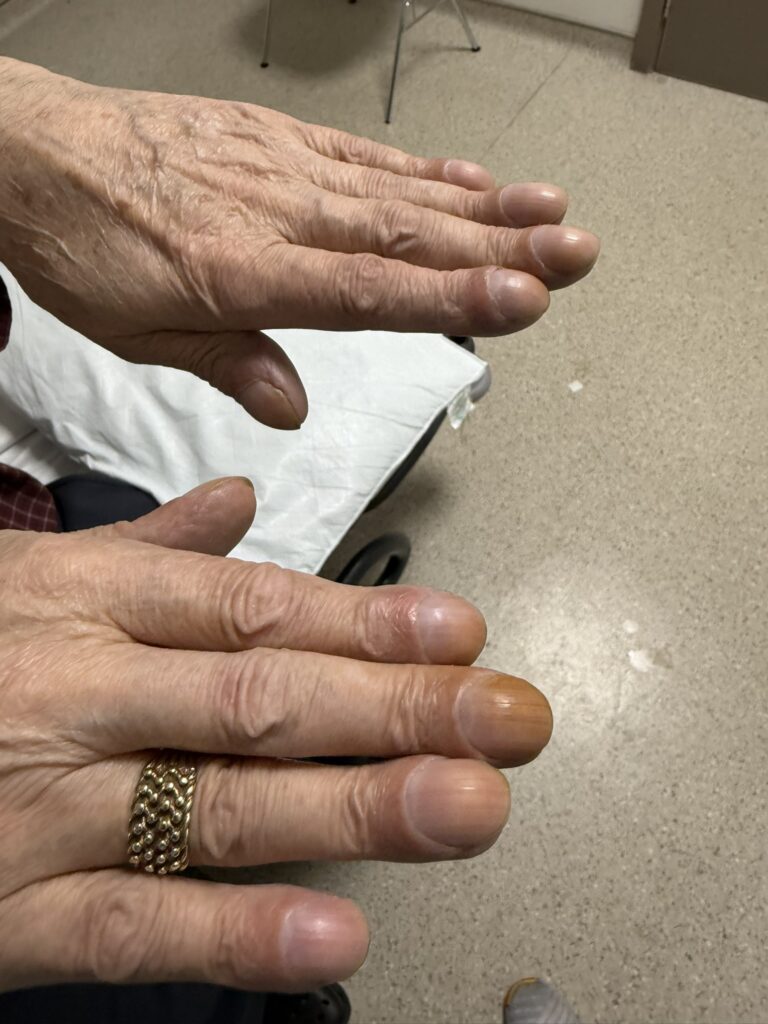
- Arachnodactyly: long, slender, spider-like fingers
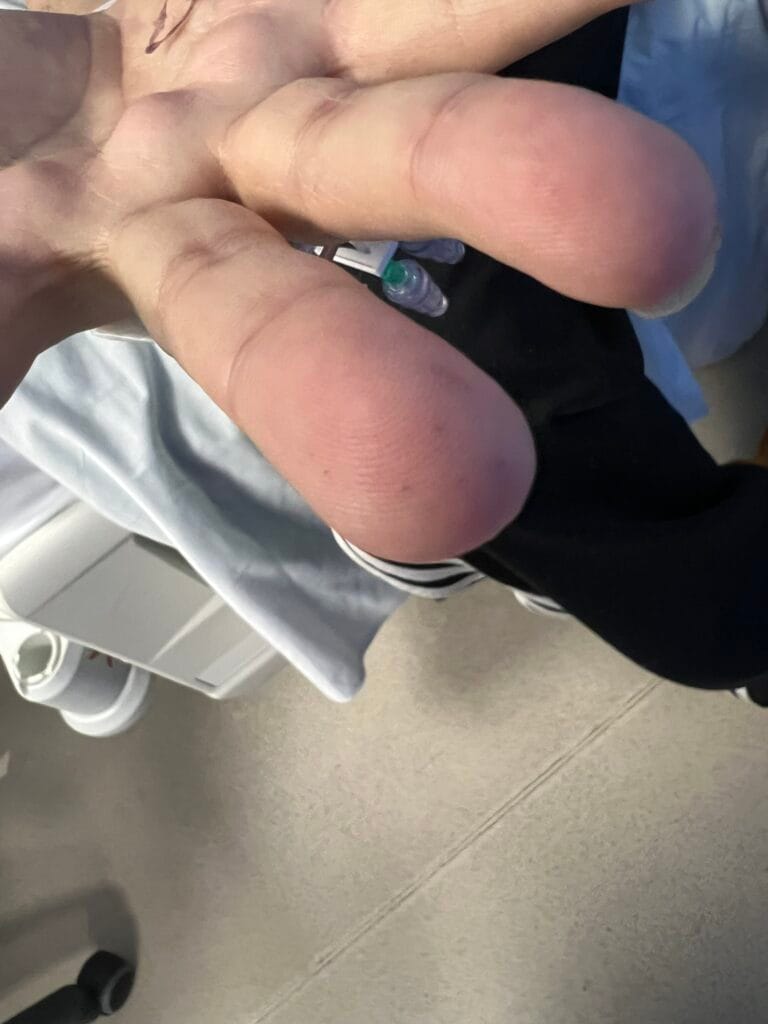
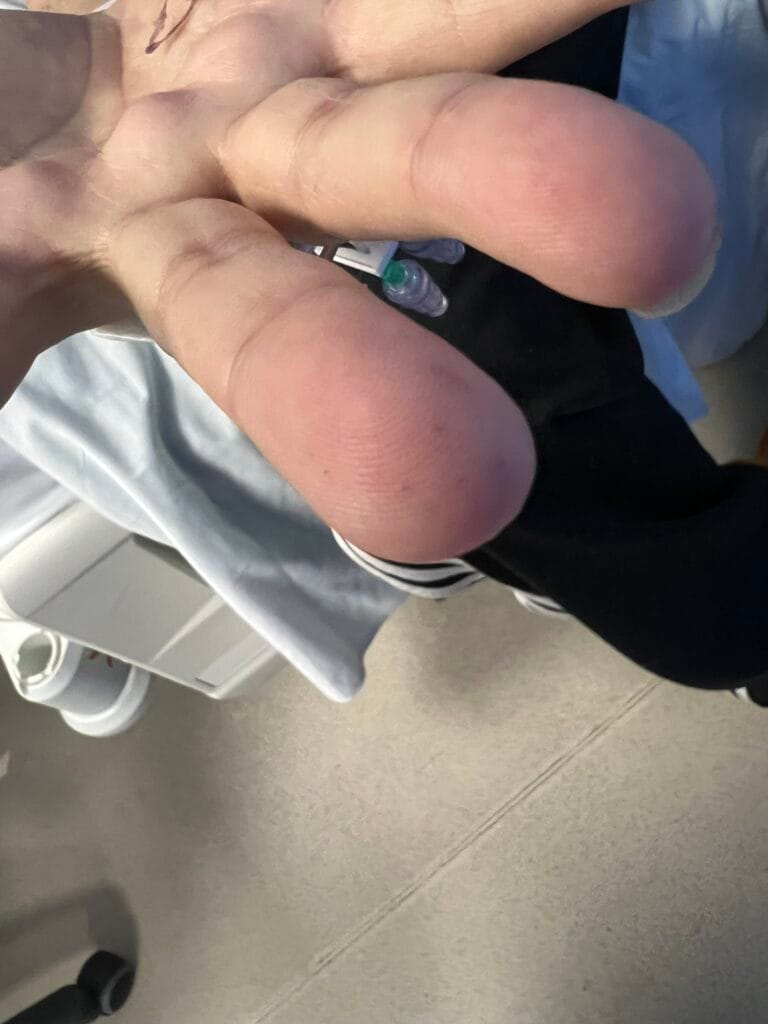
- Wrist sign (Walker sign): thumb and little finger overlap when wrapped around the contralateral wrist
- Thumb sign (Steinberg sign): thumb protrudes beyond the ulnar border of the hand when folded across the palm
- Pulse: collapsing (waterhammer) pulse — aortic regurgitation
- Peripheral stigmata of infective endocarditis: splinter haemorrhages, Osler’s nodes, Janeway lesions, clubbing
- Blood pressure: wide pulse pressure (aortic regurgitation); measure both arms (aortic dissection can cause asymmetry)
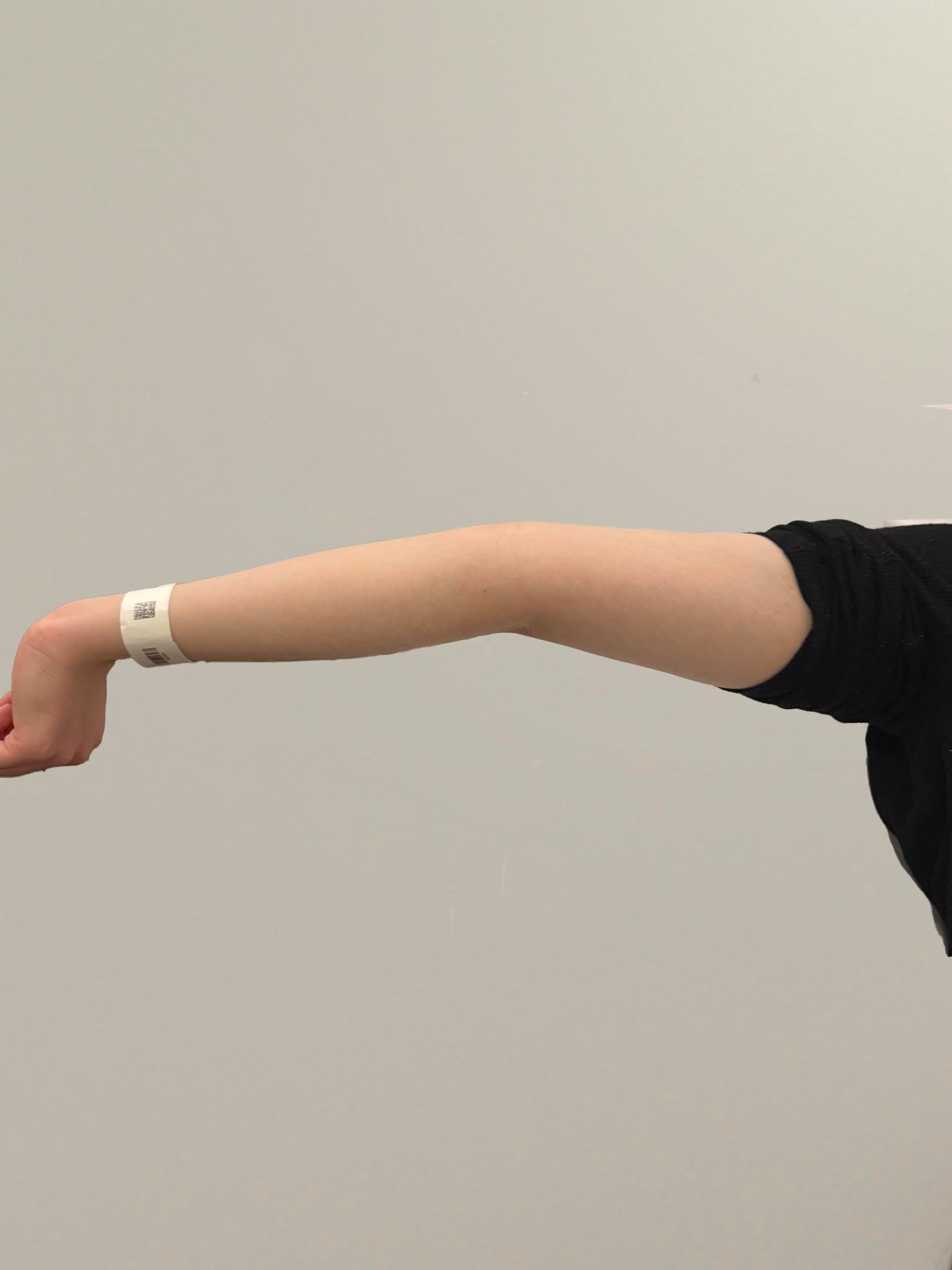
- Reduced elbow extension: limited extension is a Ghent criterion
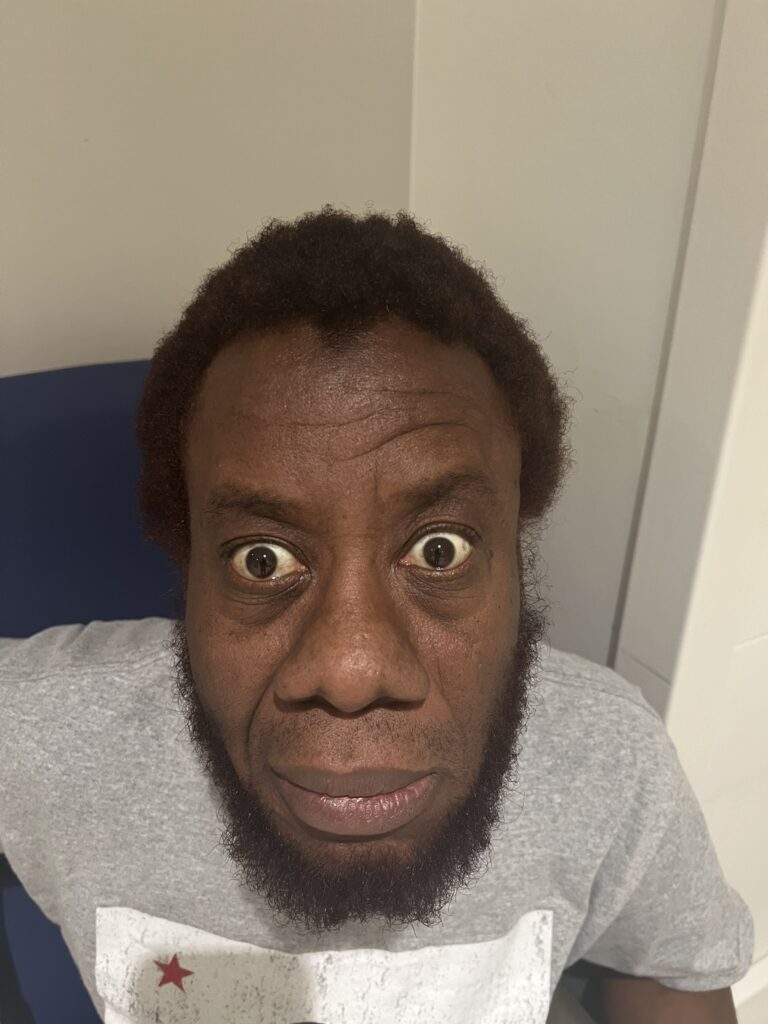
Face
- Dolichocephaly: long, narrow face
- Enophthalmos: sunken eyes
- Downslanting palpebral fissures
- Malar hypoplasia: flat cheekbones
- Retrognathia: receding chin
Eyes
- Blue sclerae
- Iridodonesis: tremulousness/vibration of the iris on eye movement — raises concern for ectopia lentis (superiorly displaced lens)
- Visual acuity: myopia is common
- Fundoscopy if visual disturbance reported (retinal detachment, optic disc changes)
- Cataract
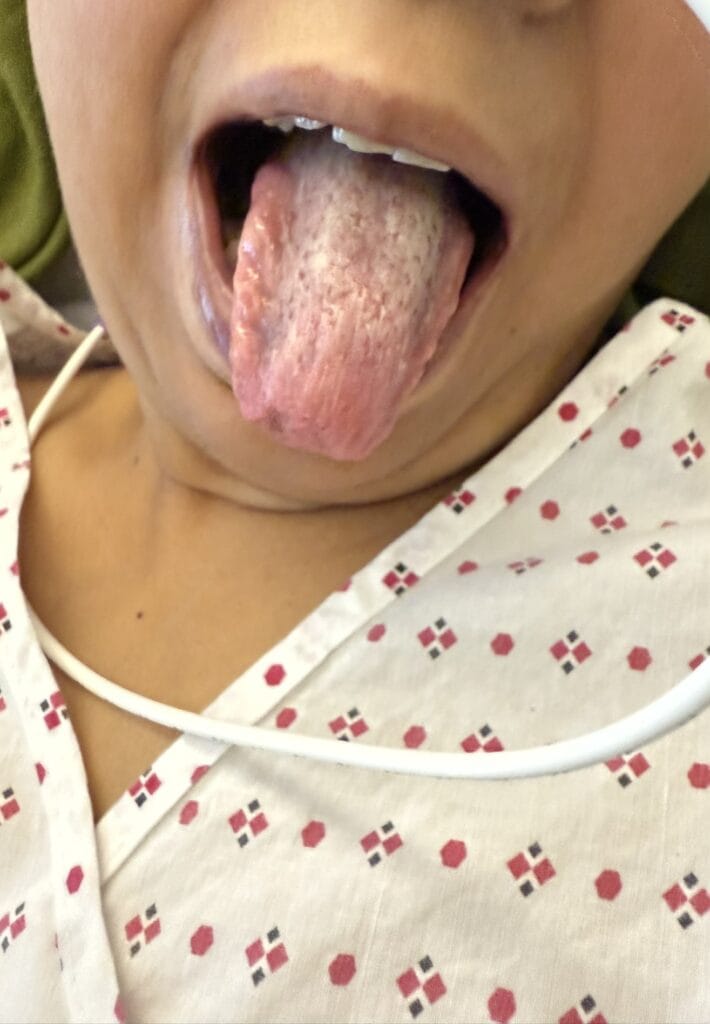
Mouth
- High-arched (gothic) palate
- Crowded teeth
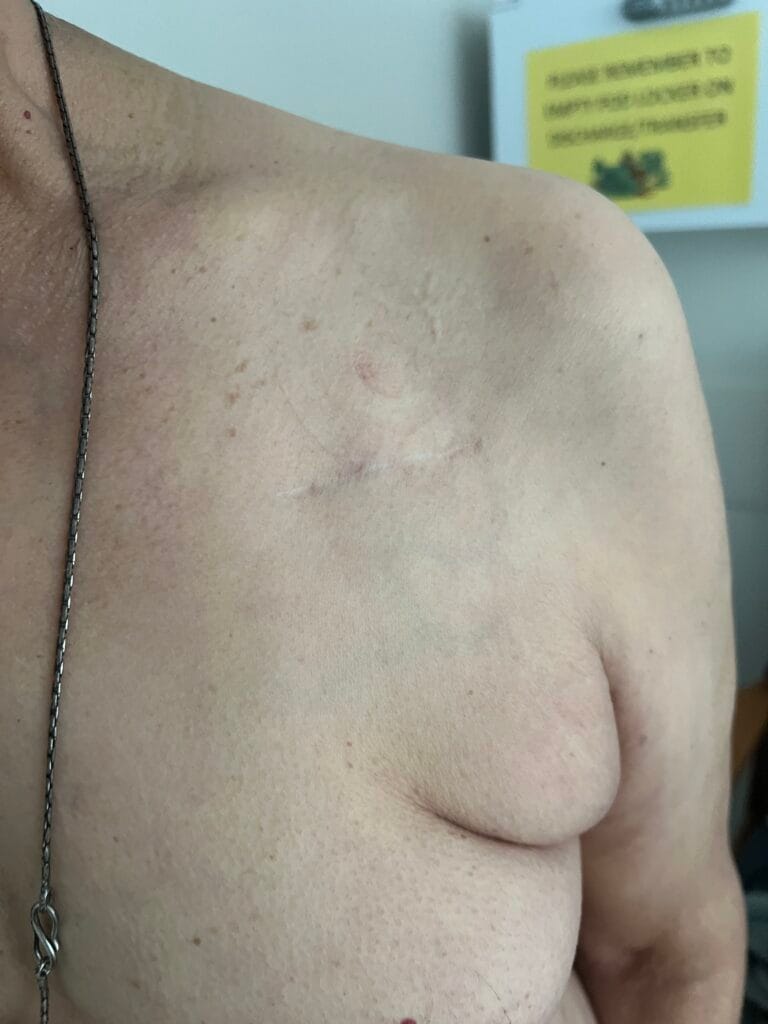
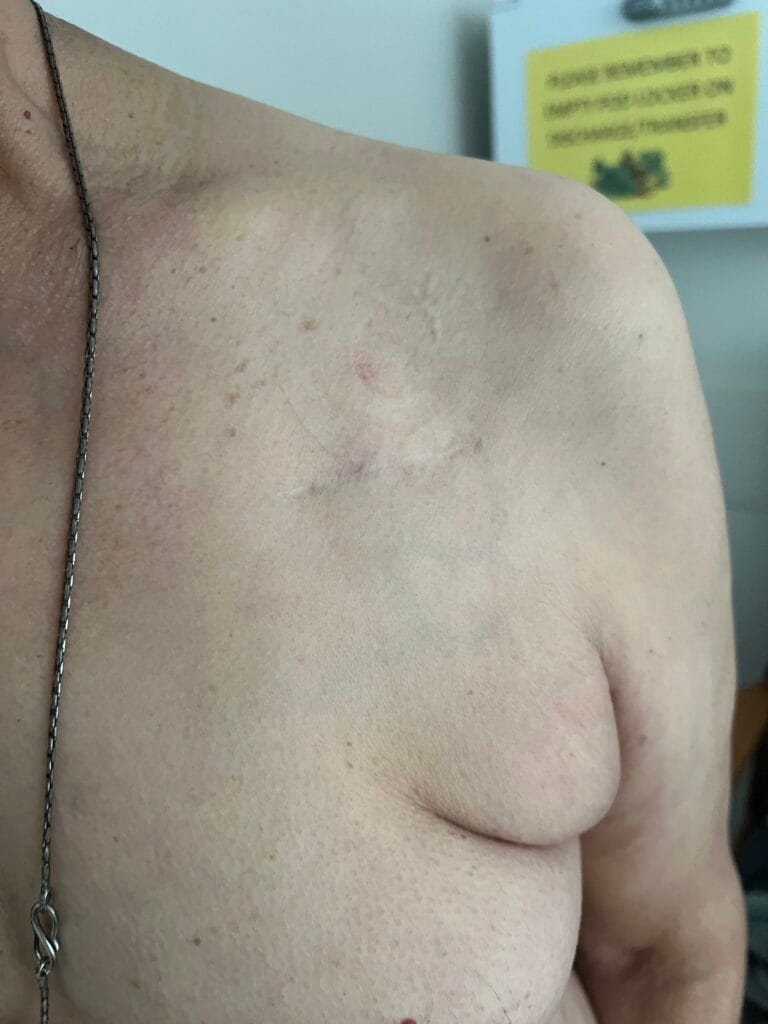
Chest
- Chest wall deformities: pectus excavatum (funnel chest) or pectus carinatum (pigeon chest)
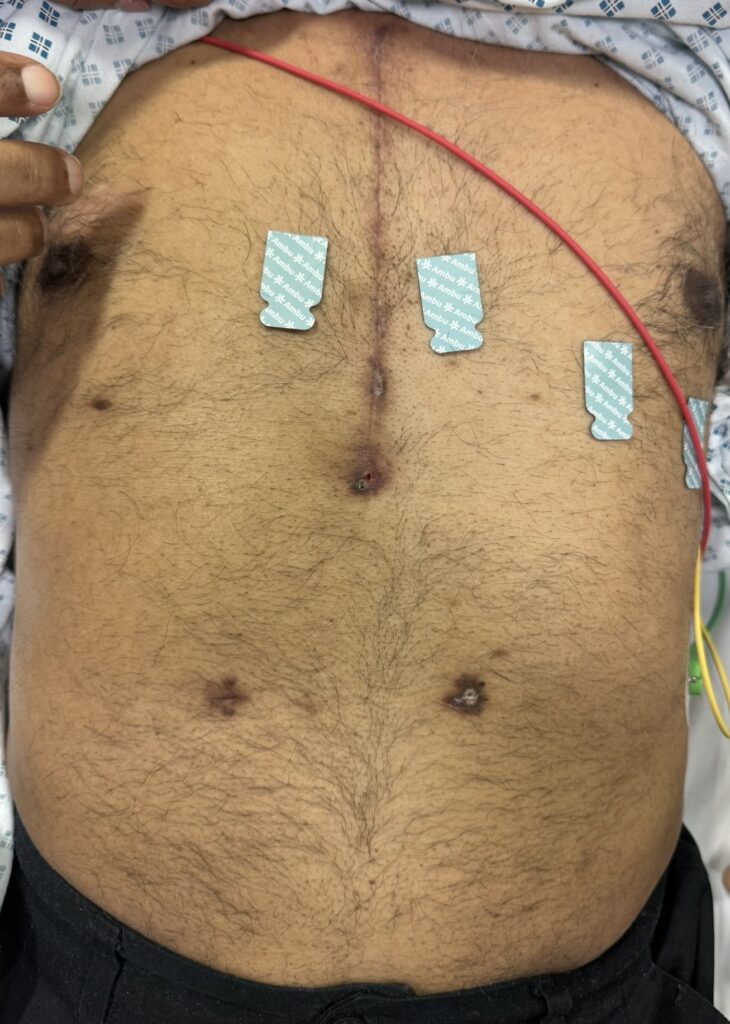
- Scars: chest drain scars (previous pneumothorax), median sternotomy or thoracotomy (aortic aneurysm/valve surgery)
- Auscultate lungs: absent breath sounds (pneumothorax)
- Auscultate heart: early diastolic murmur at left sternal edge (aortic regurgitation); mid-systolic click ± late systolic murmur (mitral valve prolapse)
Abdomen & Lower Limbs
- Striae: skin stretch marks on abdomen, thighs, back
- Offer to assess for inguinal herniae
- Protrusion acetabulae: deep hip socket (assess on imaging)
- Neurological assessment of lower limbs: power, sensation, reflexes (dural ectasia)
3. Specific Investigations
- ECG: arrhythmias, left ventricular hypertrophy (chronic AR), prolonged QT
- CXR: widened mediastinum (aortic aneurysm/dissection), pneumothorax, cardiomegaly
- Echocardiogram: aortic root diameter, aortic regurgitation, mitral valve prolapse — the single most important investigation for ongoing surveillance; annual echo recommended
- CT aorta / MRI: if dissection suspected or for detailed aortic mapping
- Slit-lamp examination: ectopia lentis (ophthalmology referral)
- Genetic testing: FBN1 mutation (chromosome 15); enables family screening
- MRI lumbosacral spine: if dural ectasia suspected (bowel/bladder symptoms, back pain)
4. Management
Specialist Referral & Surveillance
- Cardiology: annual echocardiogram to monitor aortic root diameter and rate of dilatation
- Ophthalmology: assessment for ectopia lentis, myopia, retinal detachment, cataract
- Genetics: confirm diagnosis, family screening, genetic counselling
- Orthopaedics: scoliosis, pes planus, joint hypermobility management
Cardiovascular Medical Management
- Beta-blockers (e.g. atenolol, propranolol) — reduce aortic wall stress and rate of dilatation
- Angiotensin receptor blockers (e.g. losartan) — shown to slow aortic root dilatation; used alongside or instead of beta-blockers
- Blood pressure control — strict targets to reduce aortic wall stress
Lifestyle Advice
- Avoid high-intensity exercise, contact sports, and isometric exercise (weight-lifting) — increases aortic wall stress
- Avoid activities with risk of blunt chest trauma
- Advise re: pregnancy risks (aortic dissection risk increases during pregnancy)
Surgical
- Aortic root repair / replacement: indicated when aortic root diameter ≥45 mm (or lower threshold in the presence of rapid progression, family history of dissection, or severe AR)
- Aortic valve replacement if significant aortic regurgitation
- Mitral valve repair/replacement if severe MVP with regurgitation
- Pneumothorax: chest drain if significant; surgical intervention (pleurodesis, VATS) for recurrent pneumothorax
Family Screening
- Screen all first-degree relatives with echocardiogram and clinical assessment
- Genetic testing for FBN1 mutation in affected families
Marfan’s Syndrome Cheat Sheet
| Domain | Summary |
|---|---|
| Genetics | Autosomal dominant; mutation in FBN1 gene encoding fibrillin-1 protein on chromosome 15; prevalence ~1 in 5,000; M = F |
| Systems Involved | Cardiovascular, ocular, musculoskeletal, respiratory, skin, CNS (dural ectasia) |
| Revised Ghent Criteria | Diagnosis requires: aortic root dilatation/dissection + ectopia lentis (cardinal features), or FBN1 mutation, or a sufficient systemic score (>7). Family history of Marfan’s can substitute. Systemic score features: wrist/thumb signs, pectus carinatum/excavatum, pes planus, pneumothorax, dural ectasia, protrusion acetabulae, arm span:height ratio, reduced upper:lower segment ratio, scoliosis/kyphosis, reduced elbow extension, facial features (dolichocephaly, enophthalmos, downslanting palpebral fissures, malar hypoplasia, retrognathia), striae, myopia, MVP |
| Key Examination Features | Tall, arachnodactyly (wrist and thumb signs), arm span > height, kyphoscoliosis, pes planus, pectus excavatum/carinatum, high-arched palate, dolichocephaly, blue sclerae, iridodonesis, lens dislocation (upward — contrast with homocystinuria which is downward), collapsing pulse (AR), mid-systolic click (MVP) |
| Cardiovascular Complications | Aortic root dilatation and dissection (most serious), aortic regurgitation, mitral valve prolapse ± regurgitation, infective endocarditis, arrhythmias |
| Differentials |
• Homocystinuria — downward lens dislocation, cognitive impairment, recurrent thrombosis, no cardiac involvement • MEN 2b — Marfanoid habitus, mucosal neuromas, medullary thyroid cancer, phaeochromocytoma; no eye or heart involvement • Ehlers-Danlos syndrome — skin hyperextensibility, joint hypermobility, tissue fragility; fibrillin normal • MASS phenotype — MVP, borderline non-progressive aortic dilatation, striae atrophicae, skeletal features; no ectopia lentis, no FBN1 mutation |
| Investigations | ECG; CXR (widened mediastinum, pneumothorax); echocardiogram (aortic root, AR, MVP — annual surveillance); CT/MRI aorta if dissection suspected; slit-lamp (ectopia lentis); FBN1 genetic testing; MRI lumbosacral spine (dural ectasia) |
| Management | Annual echo surveillance; beta-blockers + ARBs (slow aortic dilatation); strict BP control; avoid high-intensity/contact sport; aortic root repair if ≥45 mm; ophthalmology and genetics referral; screen first-degree relatives |
☐