Consultations
Bell’s Palsy
In Station 5 you may be asked to assess a patient presenting with a facial droop.
Station Instructions: Please assess this patient who has developed a sudden facial droop.
1. Key History-Taking Points
Timing & Character
- Onset: since when, sudden vs gradual onset, progression
- Laterality: one or both sides
- Pattern: constant vs intermittent (comes and goes)
- Previous episodes: ever happened before? (recurrent CN7 palsy is a red flag requiring further investigation)
Cranial Nerve 7 Symptoms
- Taste: loss of taste on anterior two-thirds of tongue (chorda tympani)
- Hearing: ringing in the ear (tinnitus), sensitivity to loud sounds — hyperacusis (nerve to stapedius), ache behind the ear
- Pain: facial pain or pain behind/in the ear (retroauricular pain)
- Dry eye and dry mouth: parasympathetic involvement (lacrimal and salivary glands)
- Speech: slurred speech
- Drooling
Broader Neurological Screen
- Limb symptoms: weakness or sensory loss in arms or legs (central cause, stroke)
- Facial sensation: numbness (CN5 involvement — suggests CPA lesion or brainstem)
- Headache, vomiting, seizures, personality change, weight loss, night sweats (raised ICP, malignancy)
- MS screen: tremor, Lhermitte’s sign, Uhthoff’s phenomenon, dizziness/vertigo, diplopia
- Speech, swallowing, walking, balance, vision, hearing — full cranial nerve and cerebellar symptom screen
Causes to Screen For
- Ear infection or recent otitis media (vesicles in ear canal — Ramsay Hunt syndrome)
- Head injury (petrous temporal bone fracture)
- Diabetes (mononeuritis multiplex)
- Travel history: tick exposure, wooded areas — Lyme disease (Borrelia burgdorferi)
2. Key Examination Findings
CN7 Motor Assessment
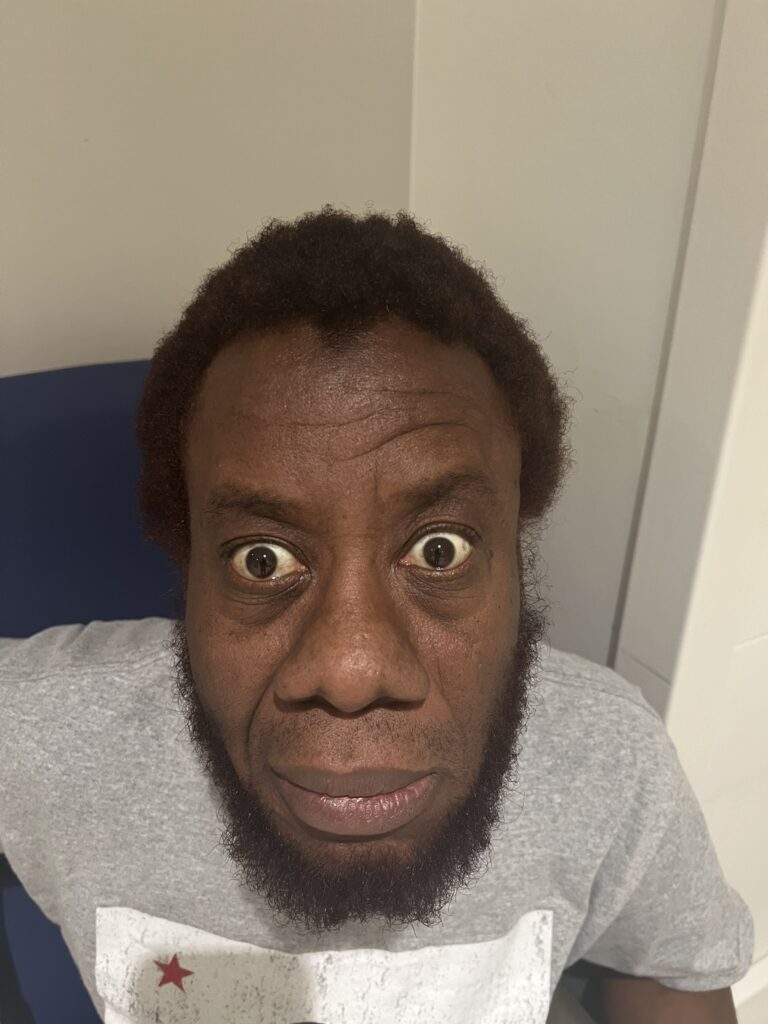
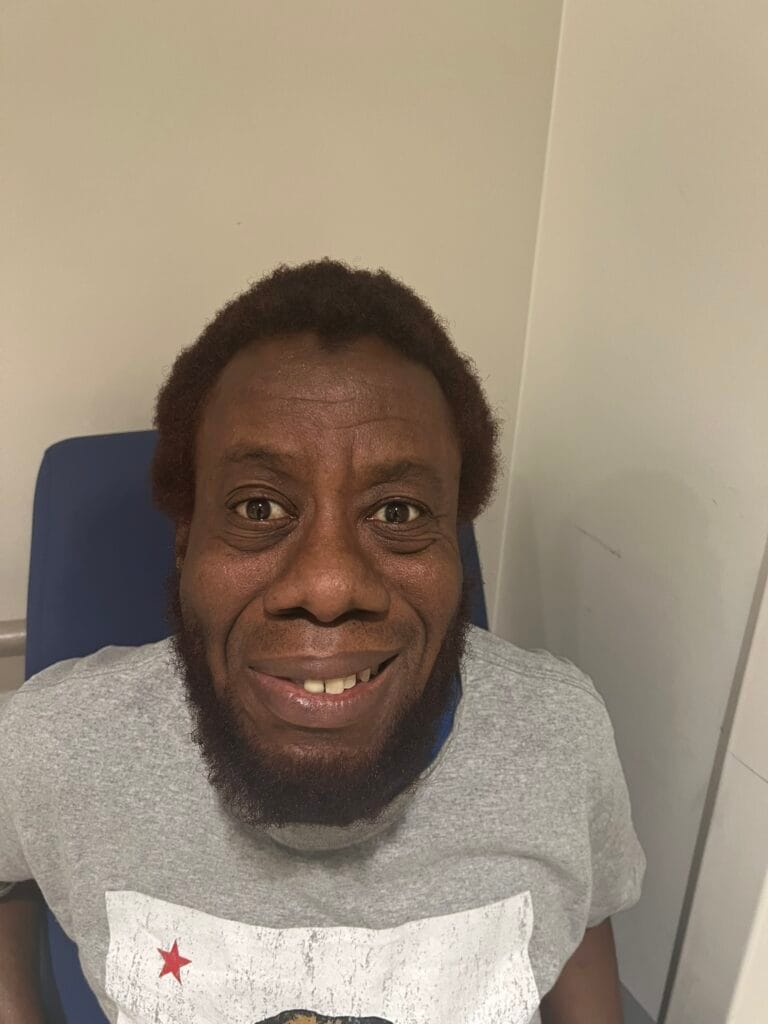
- Raise eyebrows — forehead sparing (upper motor neuron) vs complete forehead involvement (lower motor neuron = Bell’s palsy)
- Close eyes tightly — look for Bell’s phenomenon (eye rolls upward and outward on attempted closure in LMN palsy)
- Resist eye opening — test orbicularis oculi strength
- Blow out cheeks
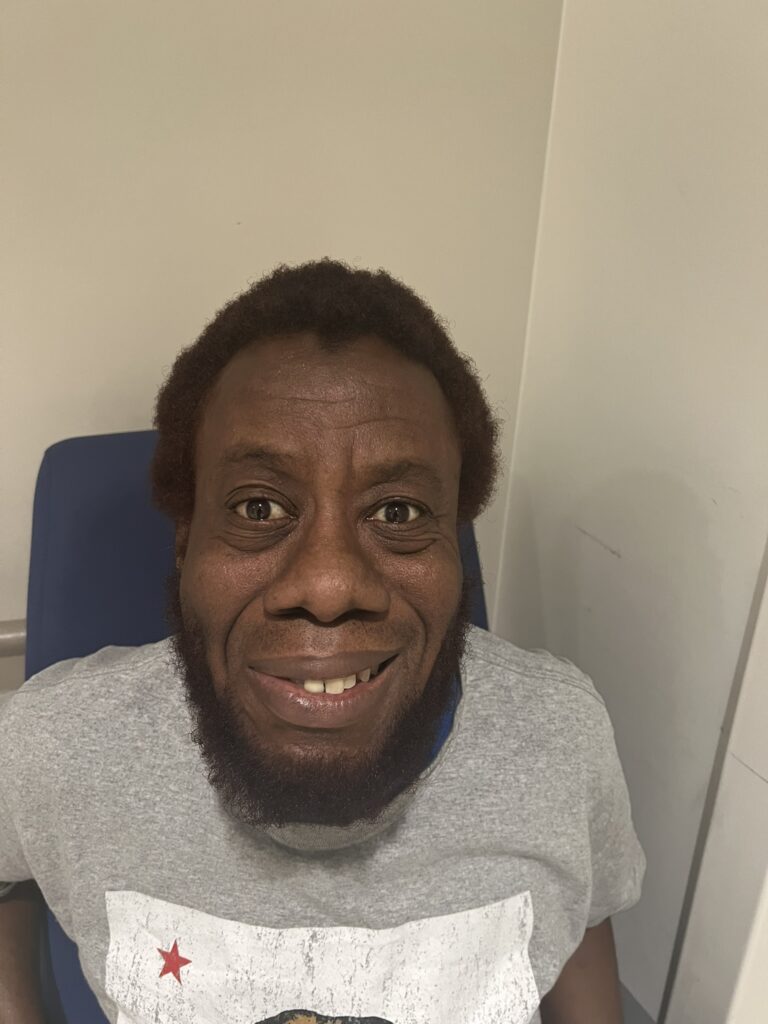
- Smile and show teeth — note lower face asymmetry
- Whistle
Complications & Treatment Signs
- Look for exposure keratopathy — corneal erythema or haziness from inability to close the eye
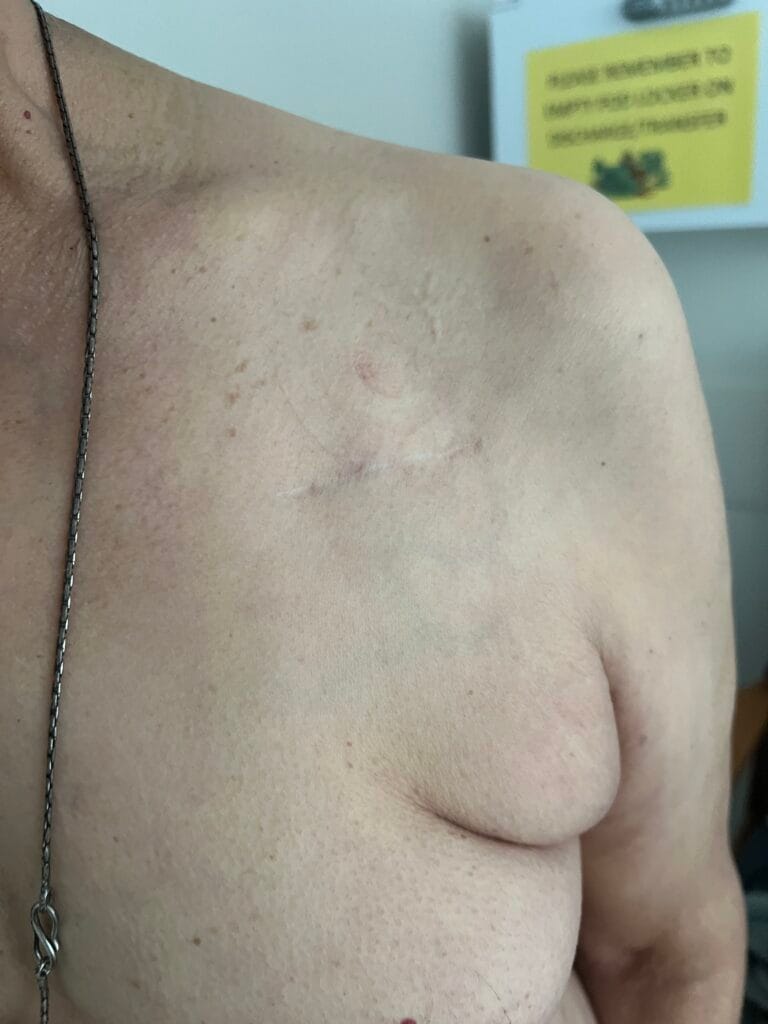
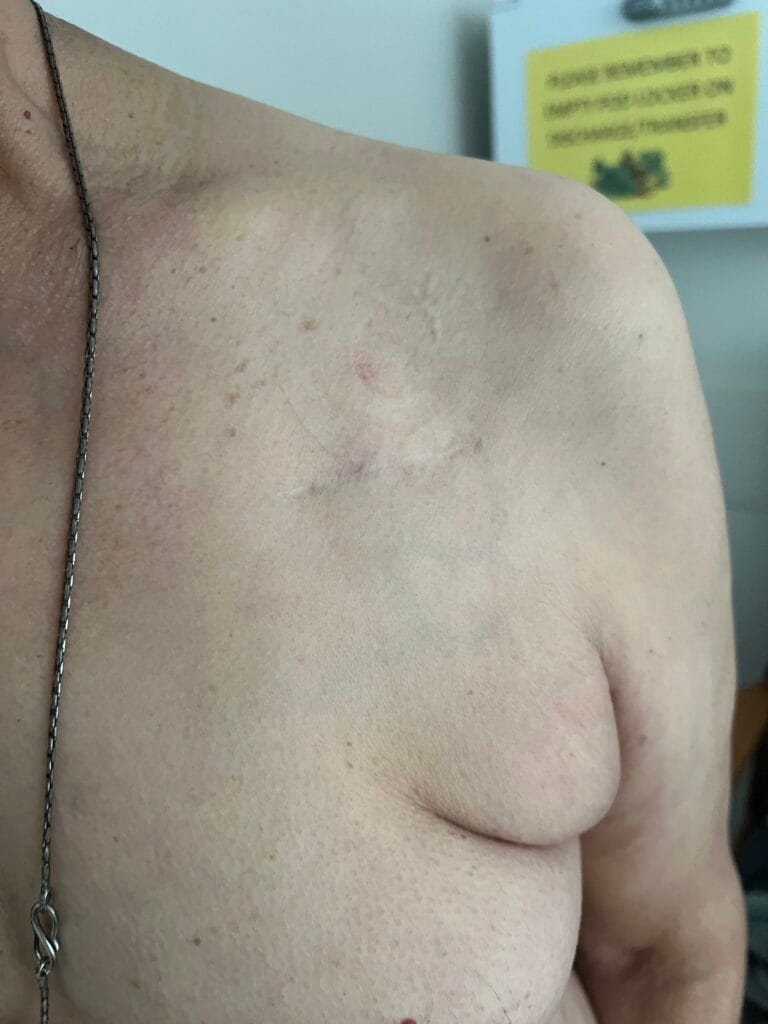
- Look for evidence of treatment: tarsorrhaphy scar (surgical lid closure to protect cornea)
- Synkinesis — abnormal co-contraction of facial muscles (late complication of aberrant nerve regeneration)
Other Cranial Nerves
- CN 3, 4, 6: pupils, eye movements (diplopia)
- Visual fields and fundoscopy (papilloedema, optic atrophy)
- CN 5: facial sensation in all three divisions
- CN 8: hearing (whisper test, Weber and Rinne)
Neurological Examination
- Upper and lower limb tone, power, coordination, sensation (screen for central lesion)
- Upper limb examination for myelopathy if indicated
Targeted Local Examination
- Ear: look for vesicles in the ear canal and pinna (Ramsay Hunt syndrome — herpes zoster reactivation), cholesteatoma, signs of otitis media
- Mouth: vesicles on palate or mucosa
- Scars: behind the ear or within the hairline (mastoid/parotid surgery)
- Parotids: palpate for enlargement or mass (parotid tumour, sarcoid, mumps)
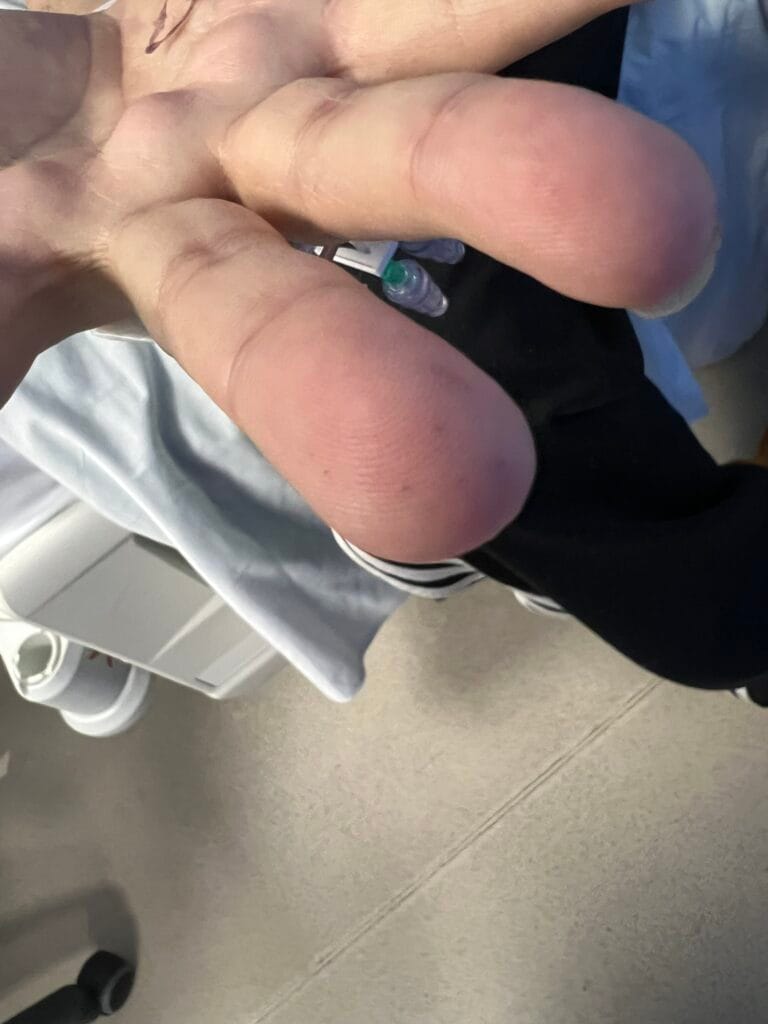
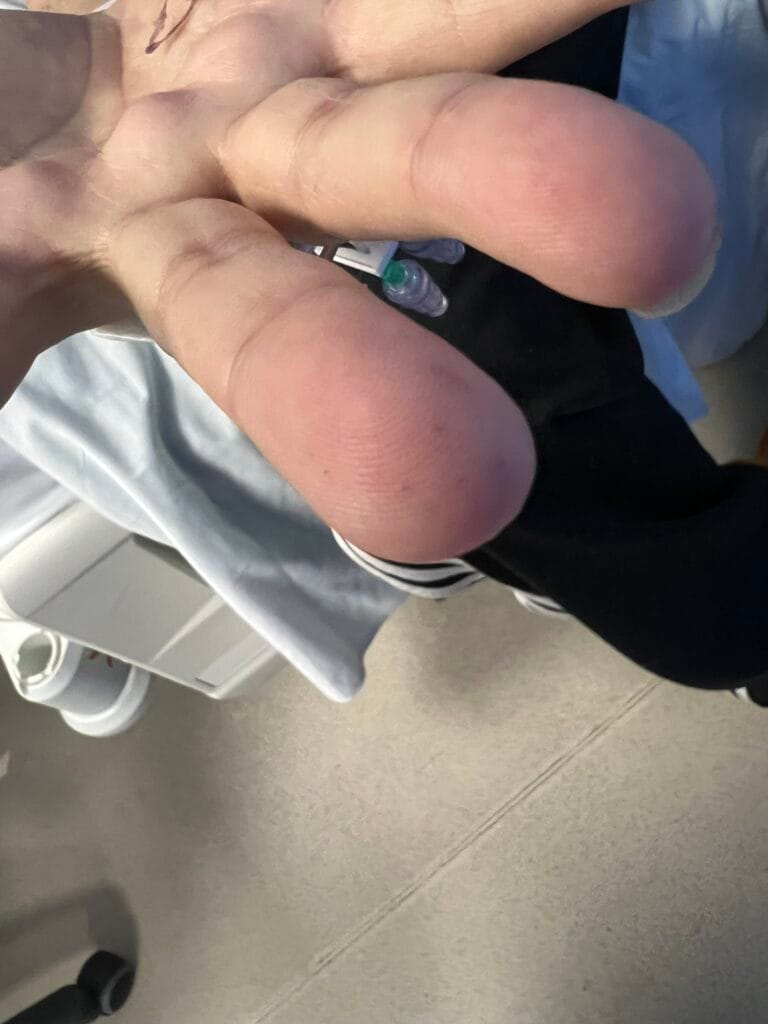
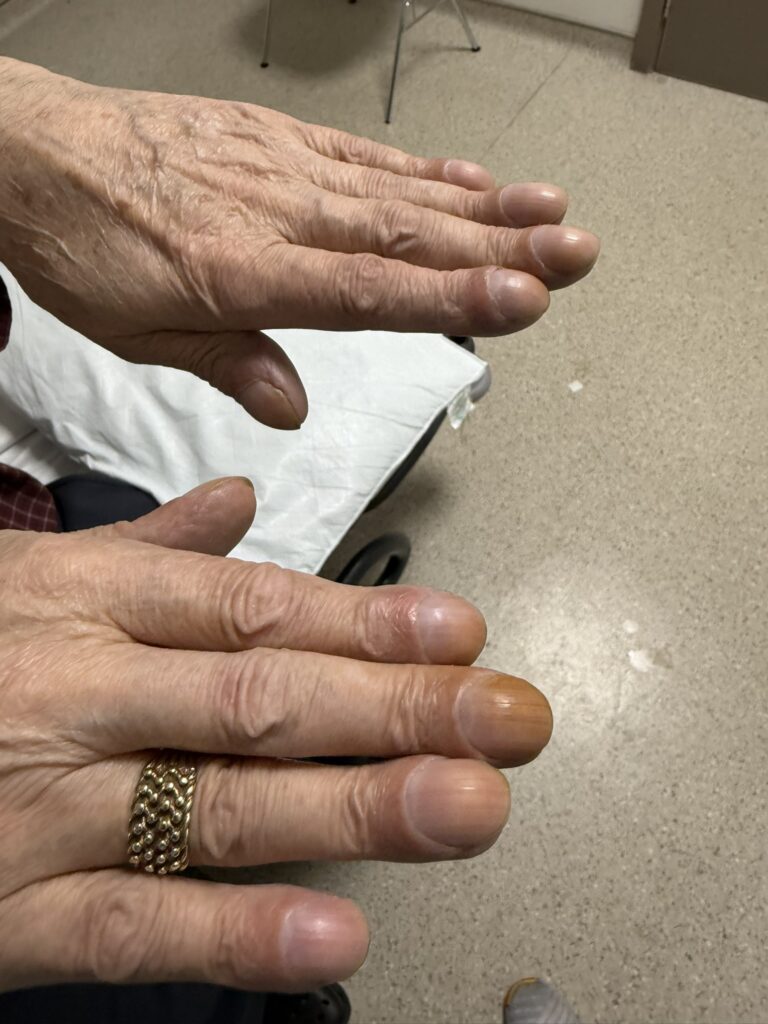
- Hands: fingerprick marks (capillary blood glucose testing for diabetes), vasculitic signs (mononeuritis multiplex)
ICE explanation template: “There are many reasons for weak face muscles. The most likely cause is a problem with the facial nerve — this is often viral. Most patients make a full recovery within 2–3 months, though it can take up to 6 months and some weakness may persist. I will give you steroids for 10 days: 50 mg for 5 days, then tapering by 10 mg every day. I’ll also arrange an eye patch, lubricating eye drops and ointment, and analgesia, and give you a leaflet on facial massage. There is around a 1 in 10 chance of recurrence. I don’t think this is a stroke or tumour because your forehead muscles are affected — a stroke spares the forehead — and a tumour would cause a slower progression. I will check your blood pressure, examine your eyes and ears thoroughly, and arrange blood tests including glucose, cholesterol, and inflammatory markers. I’ll refer you to a neurologist and ask you to contact us immediately if you develop any new symptoms.”
3. Specific Investigations
If Isolated Lower Motor Neuron CN7 Palsy (Bell’s Palsy Likely)
- Blood pressure
- Fasting glucose (diabetes)
- Fasting lipids
- ESR, FBC (inflammatory screen)
- Lyme serology (ELISA ± Western blot) if travel to endemic area or tick exposure
If Red Flags Present (Brainstem / Other CN Signs / Bilateral / Recurrent / Slowly Resolving)
- MRI brain, petrous temporal bone and parotid gland
- CT head if MRI unavailable or bony detail needed
- Autoimmune screen: ANA, ANCA, complement
- HIV test
- Blood film, LDH, immunoglobulins (haematological malignancy)
- Serum ACE (sarcoidosis)
- Lyme serology if indicated
4. Management
Acute Treatment
- Corticosteroids: prednisolone 50 mg daily for 5 days, then tapered (40, 30, 20, 10, 5 mg) — start within 72 hours of onset for maximum benefit
- Antivirals: aciclovir may be added if Ramsay Hunt syndrome suspected (herpes zoster reactivation)
- Eye protection: lubricating eye drops (daytime), eye ointment (night), eye patch — critical to prevent exposure keratopathy
- Analgesia
- Facial massage: patient education leaflet; physiotherapy referral
Follow-Up & Referral
- Neurology referral
- Ophthalmology referral if corneal involvement or incomplete eye closure persists
- Tarsorrhaphy (surgical partial lid closure) if exposure keratopathy is refractory
- Advise patient to return immediately if new symptoms develop
- Warn of 10% recurrence risk
Treat Underlying Cause if Identified
- Antibiotics for Lyme disease (doxycycline or amoxicillin)
- Antifungals/antibiotics for otitis media or cholesteatoma
- Treat diabetes, sarcoidosis, vasculitis as appropriate
Bell’s Palsy Cheat Sheet
| Domain | Summary |
|---|---|
| Definition | Acute peripheral facial palsy of unknown cause; named after Sir Charles Bell; HSV-1 reactivation is the likely cause in most cases; M = F, any age; sudden onset and progressive |
| UMN vs LMN | LMN lesion (e.g. Bell’s palsy): entire ipsilateral face affected including forehead. UMN lesion (e.g. stroke): forehead spared due to bilateral cortical innervation of forehead muscles — forehead sparing = upper motor neuron |
| CN7 Course | Nucleus in the pons → fibres loop around CN6 nucleus → emerges at cerebellopontine angle → enters internal auditory meatus with CN8 → geniculate ganglion → facial canal in petrous temporal bone → exits stylomastoid foramen → parotid gland → terminal branches |
| Causes by Location |
Pons: stroke, SOL, demyelination (MS) Base of skull: infection (Lyme, TB), infiltration, vasculitis Cerebellopontine angle: acoustic neuroma, meningioma, neurofibroma Petrous temporal bone: Bell’s palsy, Ramsay Hunt, otitis media, cholesteatoma, tumour Parotid: tumour, sarcoid, mumps, surgery, Lyme Other: mononeuritis multiplex (diabetes, vasculitis) |
| Features of Bell’s Palsy | Retroauricular pain; hyperacusis (stapedius); reduced taste anterior ⅔ tongue (chorda tympani); dry eye and mouth (parasympathetic); Bell’s phenomenon on attempted eye closure; often painless; full LMN pattern |
| Bilateral CN7 Palsy | Myasthenia gravis, myotonic dystrophy, facioscapulohumeral dystrophy, Guillain-Barré syndrome, sarcoid, Lyme disease, MND, vasculitis, bilateral Bell’s, bilateral CPA tumours, bilateral pontine lesions, bilateral parotid pathology |
| Complications | Exposure keratopathy, taste loss, synkinesis (aberrant regeneration), residual weakness, facial contracture |
| Investigations | Isolated LMN: BP, glucose, lipids, ESR, FBC ± Lyme serology. Red flags: MRI brain/temporal bone/parotid, autoimmune screen, HIV, blood film/LDH/immunoglobulins, ACE |
| Management | Prednisolone (50 mg tapering over 10 days, start within 72 hrs); eye protection (drops, ointment, patch); analgesia; facial massage; neurology ± ophthalmology referral; treat underlying cause; warn of 10% recurrence |
☐