Skip to content
Home
Stations
Respiratory Station
Cardiology Station
Neurology Station
Abdominal Station
Communication Station
Consultations
Top Tips
Exam Centre Analysis
PACESAid Case Meta-Analysis
PACESAid Meta-Analysis Results
Join Us
Log In
Membership Account
Home
Stations
Respiratory Station
Cardiology Station
Neurology Station
Abdominal Station
Communication Station
Consultations
Top Tips
Exam Centre Analysis
PACESAid Case Meta-Analysis
PACESAid Meta-Analysis Results
Join Us
Log In
Membership Account
End of Life and Palliative Care
Membership Required
You must be a member to access this content.
View Membership Levels
Already a member?
Log in here
Mitral Stenosis Auscultation
×
Early decrescendo diastolic murmur
×
Audible Click
×
Arm Length Span
×
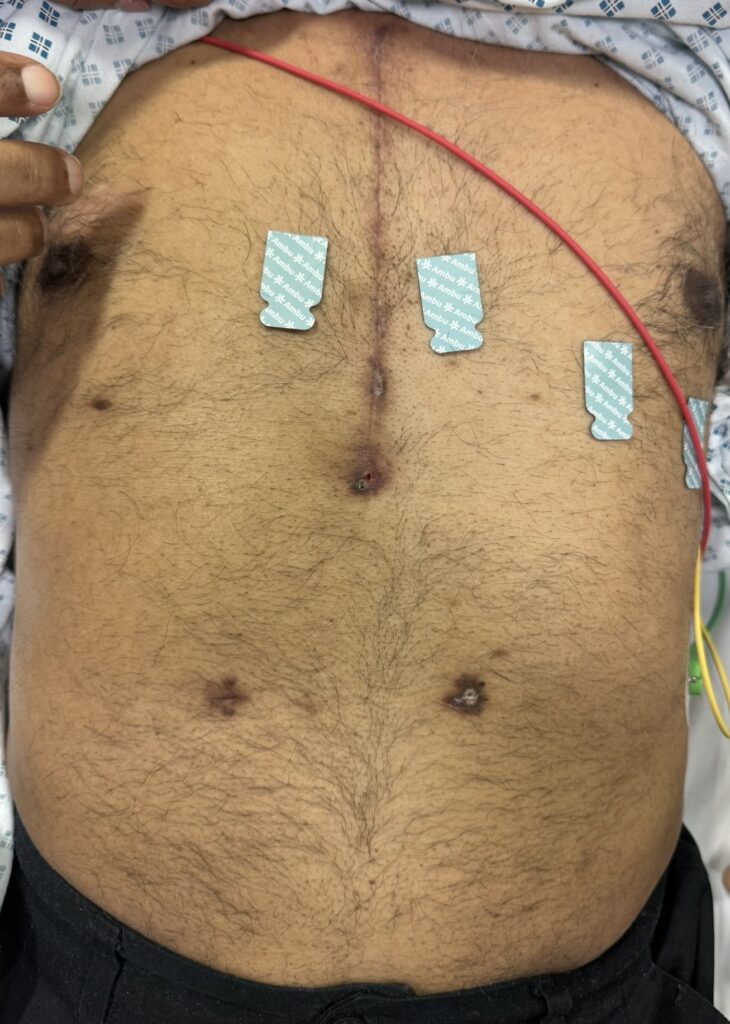
Second midline sternotomy scar
×
Splinter Haemorrhages
×
Muscle wasting
×
Loss of forehead wrinkles unilaterally (LMN disease)
×
Asymmetry
×
JVP
×
Fine Tremor Beta Agonist
×
VAT Scars
×
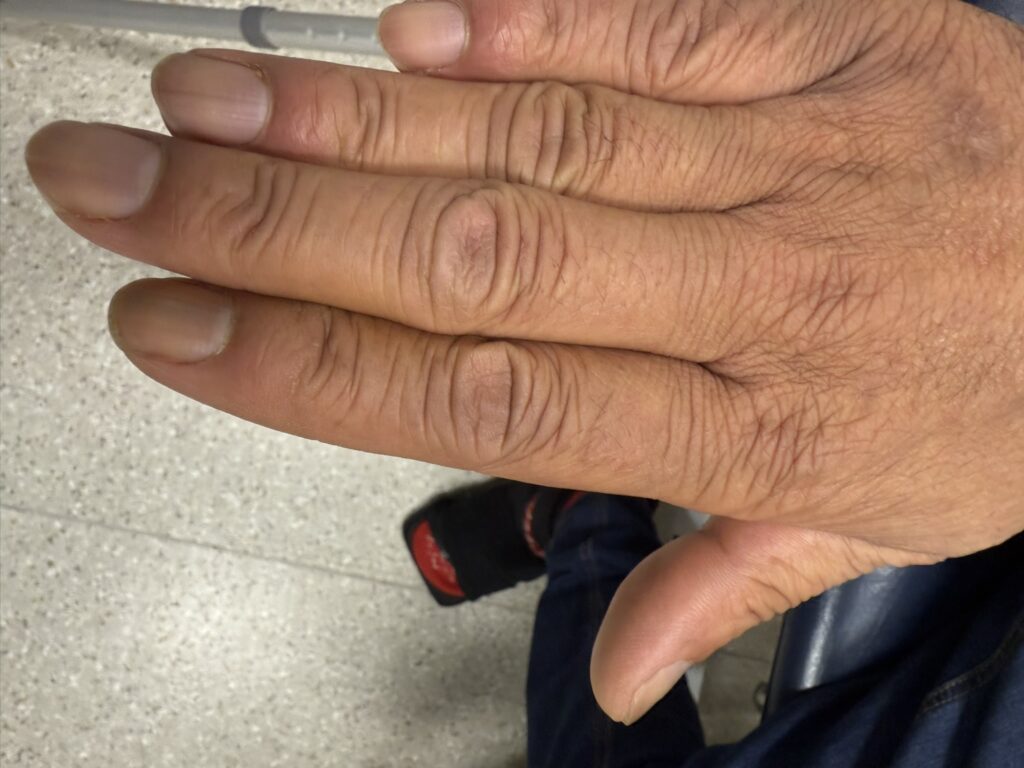
Terminal Phalanx Tufting
×
Arteriovenous Fistula
×
Mercedes-Benz
×
Inverted J-Shape Scar
×
Segmentectomy Scar
×
Chest Drain Scar and VAT scars
×
Lip Telangiectasia
×
Face Telangiectasia
×
Chest Drain Scar and VAT scars
×
Tar Stained Fingers
×
Pes Cavus
×
Infantile Hemiparesis
×
Hair loss shiny skin (diabetic neuropathy)
×
Foot deformity
×
Foot Deformity (Charcot joint)
×
Amputations
×
Pes Cavus
×
Motor Neurone Disease Muscle Wasting
×
Motor Neurone Disease Arm Muscle Wasting
×
Hypothenar Wasting Claw Hand
×
Hyperflexibility
×
Hyperextended Elbow
×
High Arched Palate
×
Finger Hyperextension
×
Arm Span Length
×
Renal Transplant Scar
×
Peritoneal Dialysis Scars
×
Parathyroidectomy Scar
×
Maturing Arteriovenous Fistula
×
Maturing Arteriovenous Fistula
×
Inspiratory Crackles Superior Aspect Pleural Effusion
×
Increased Tone Hypertonia
×
Extensor Plantars
×
Ankle Clonus
×
Resting pill rolling tremor
×
Peripheral Oedema
×
Renal Transplant Scar
×
Flanks
×
Liver Transplant Scar and Drain Scar
×
Pansystolic Murmur
×
JVP CV Waves
×
JVP Rise
×
Double Metallic Valve Auscultation
×
Aortic Valve Replacement
×
Mitral Valve Replacement
×
Aortic Stenosis
×
Bradykinesia decreasing amplitude
×
Myotonia
×
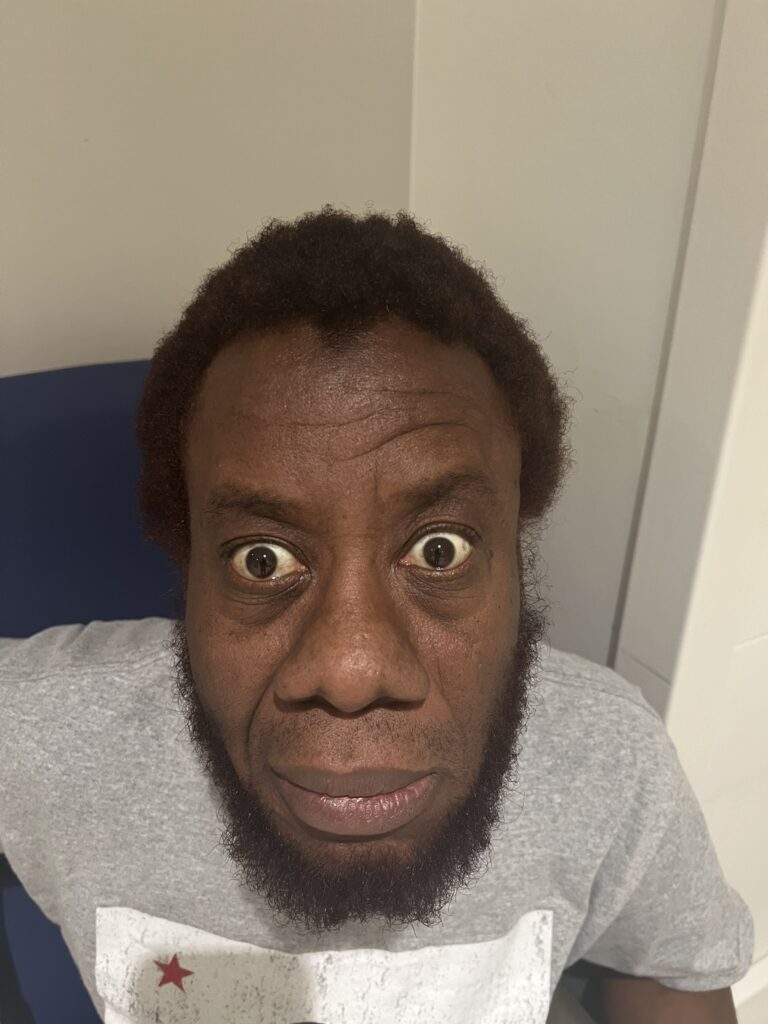
Delayed eye opening
×
Upgoing Plantars
×
Saccade
×
Nystagmus
×
Dysdiachokinesia
×
Dysmetria
×
Intention Tremor
×
Heel to Shin
×
Ataxic
×
Fine End Inspiratory Crackles
×
Wheeze
×
Expiratory Wheeze
×
Spider Naevi Refilling
×
Fine Tremor
×
Asterixis Flap
×
Nephrectomy scar
×
Xerosis and Diabetic Dermopathy
×
Toe ulcer
×
Shiny Skin and Hair Loss
×
Ichthyosiform skin changes scaling dryness
×
Diabetic Dermopathy
×
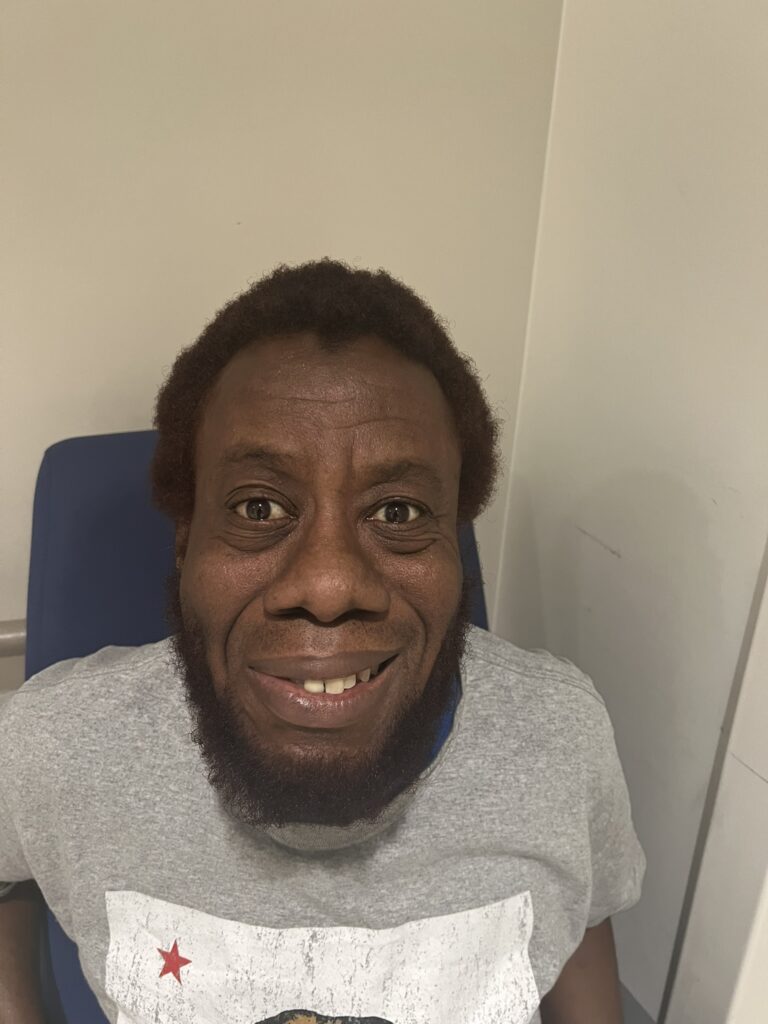
Myotonic Facies - Ptosis, Frontal Balding, Masseter wasting, Long thin face
×
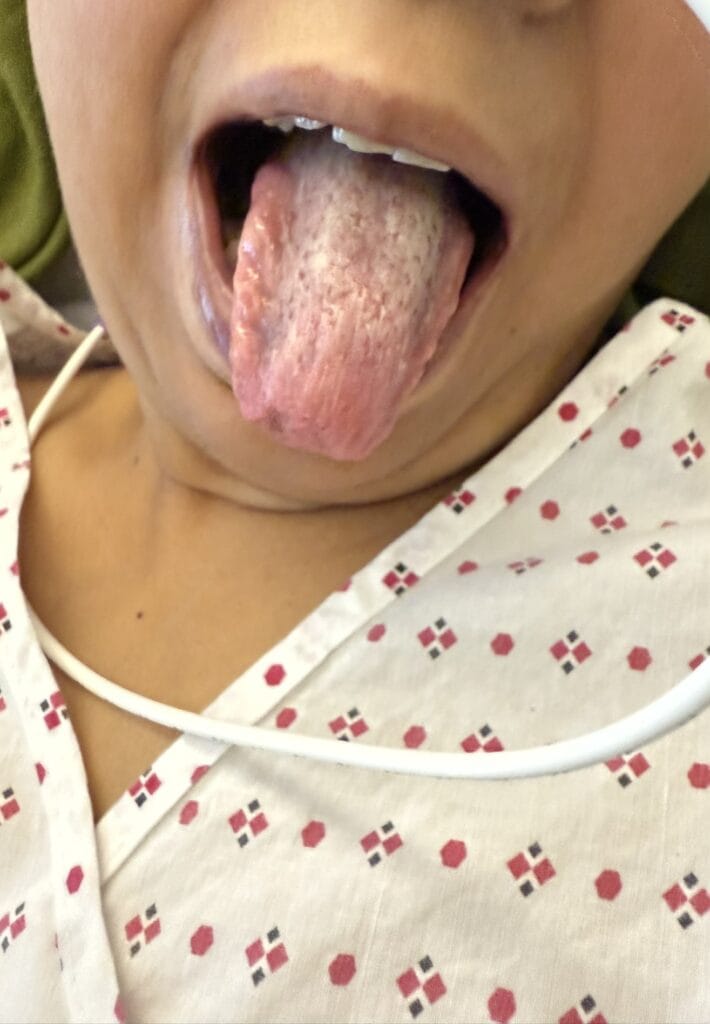
Tongue Wasting
×
Thenar Eminence Wasting
×
Dorsal Interosseous Muscle Wasting
×
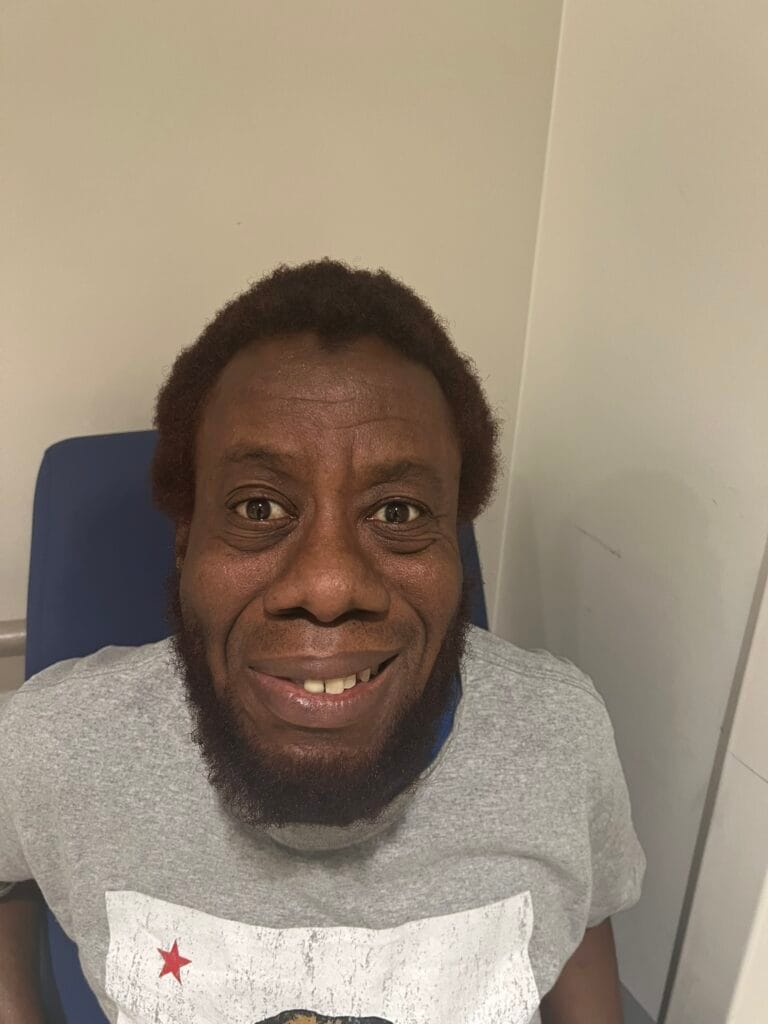
Right-sided Facial Weakness
×
Eye Closure Weakness
×
Warfarin Bruising
×
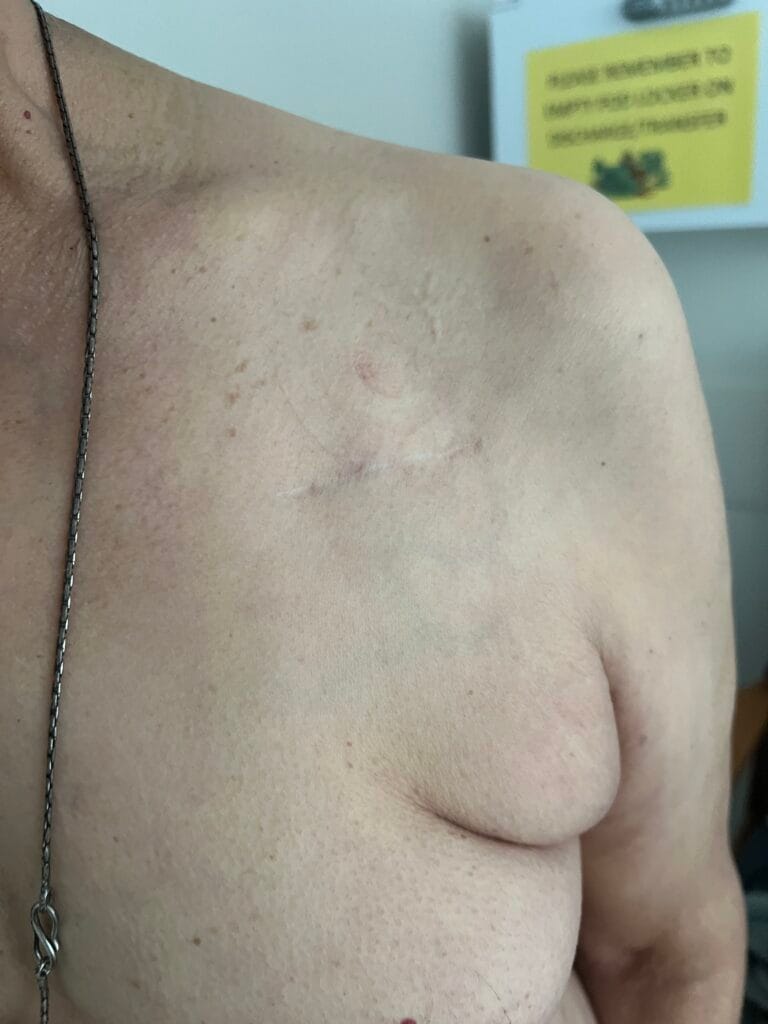
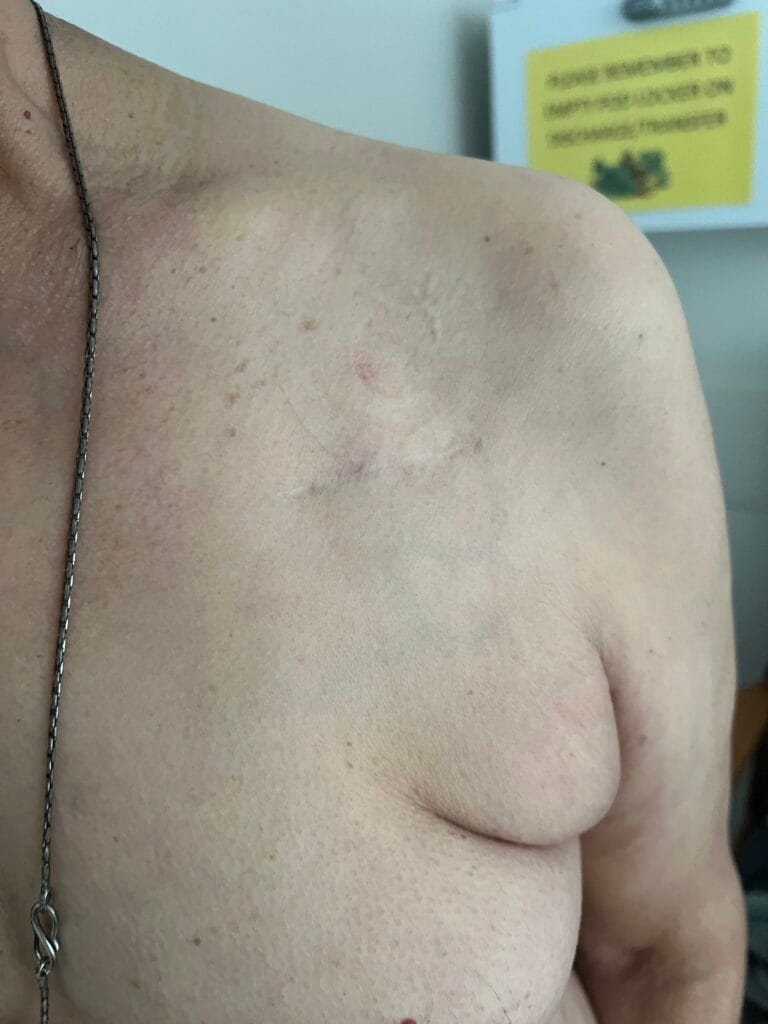
Midline Sternotomy Scar
×
Infraclavicular Cardiac Device Scar
×
Permanent Pacemaker Sinus Node Dysfunction
×
Midline Sternotomy Scar
×
Leg Vein Harvesting Scar
×
Infraclavicular Cardiac Device Scar
×
Warts
×
Peritoneal Catheter
×
Parathyroidectomy Scar
×
Glucose Monitoring Fingerprick Marks
×
Central Venous Catheter Scars
×
Arteriovenous Fistula Active Needling
×
Palmar Erythema
×
Liver Transplant Scar
×
Jaundice
×
Gynaecomastia
×
Glucose Monitoring Fingerprick Marks
×
Dupuyten contracture
×
Axillary Hair Loss
×
Ascites with umbilical hernia
×
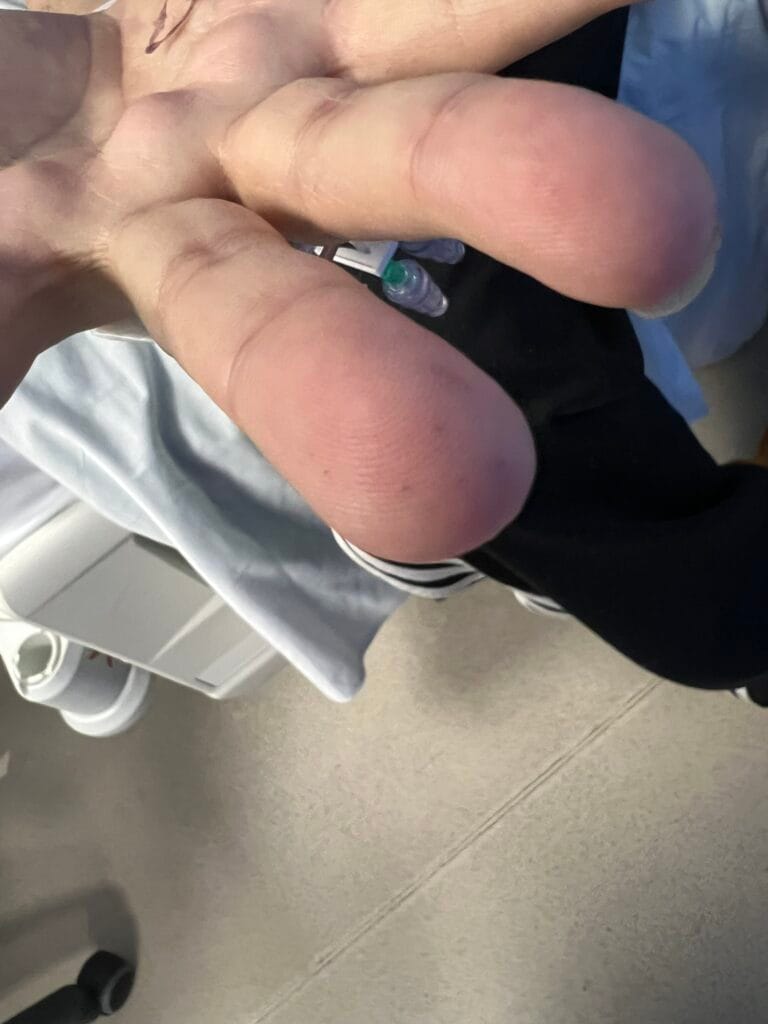
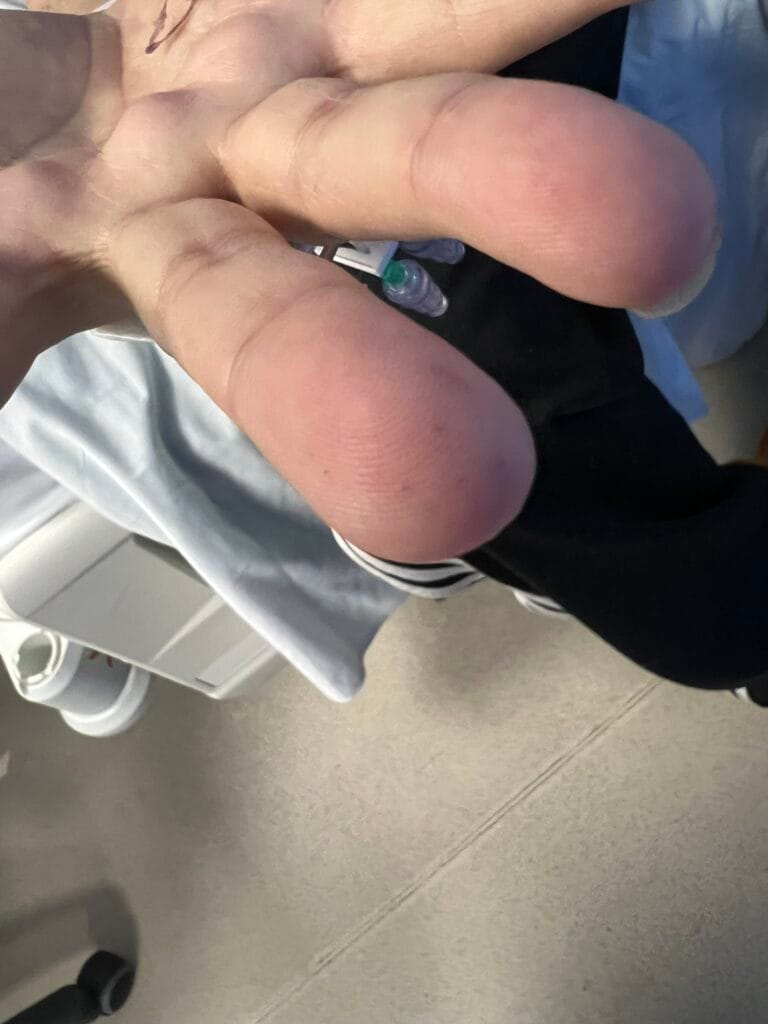
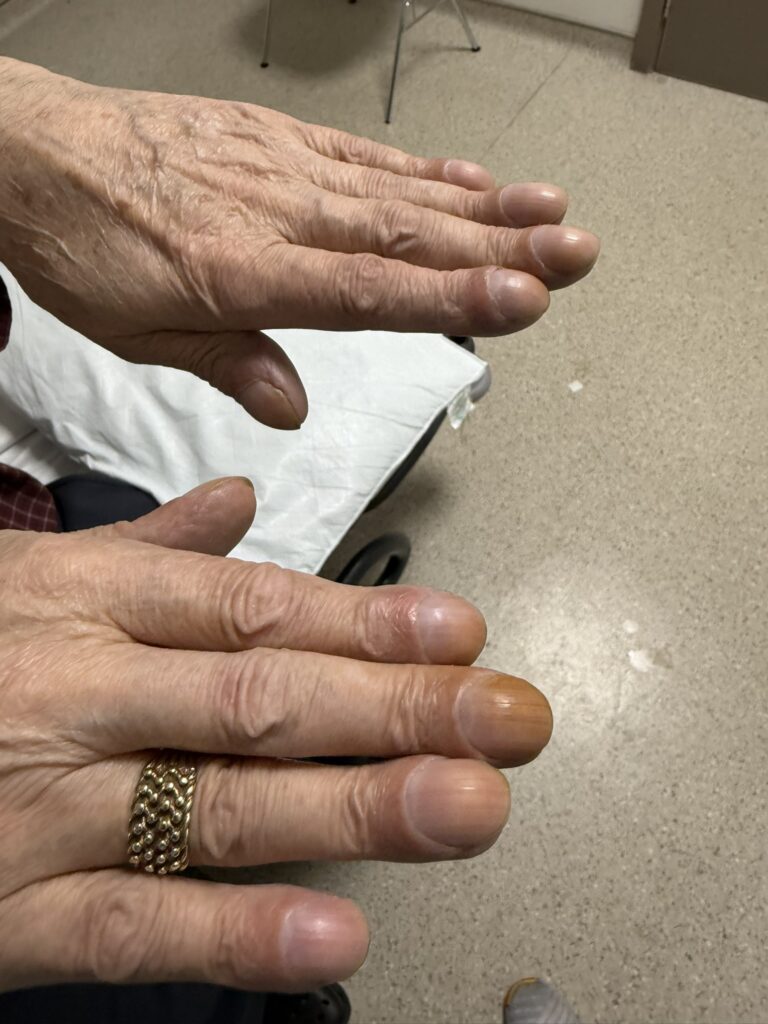
Clubbing
×
VAT Scars and Chest Drain Scar
×
VAT Scar lobectomy
×
Sclerodactyly
×
Fine-End Inspiratory Crackles
https://pacesaid.com/wp-content/uploads/2024/11/Fine-End-Inspiratory-Crackles-Made-with-Clipchamp_1731434392624-1.mp4
×
Microstomia
×
Raynauds
×
Clubbing
×
Tar staining
×